This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In many emergency departments (ED), US machines are readily available and can be used to rapidly assess and monitor patients with acute dyspnea at the bedside. What They Did: Design: Randomized, controlled, blinded-outcome trial Sites: Three emergency departments in Denmark Duration: October 9, 2019 to May 26, 2021.
I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I had only 9 false positives but I missed 2 OMI. The rhythm for the ECG in Figure-1 is sinus — with normal intervals and axis ( mean QRS axis about +80 degrees ). Time is myocardium.
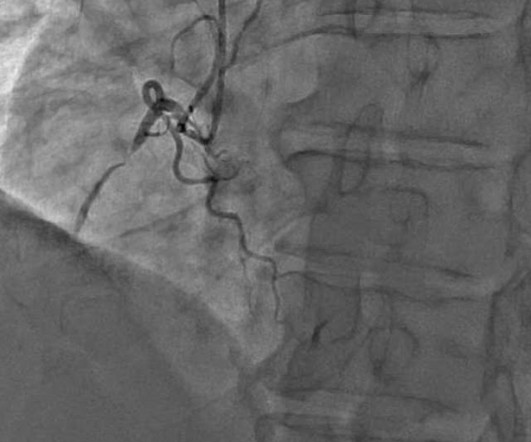
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
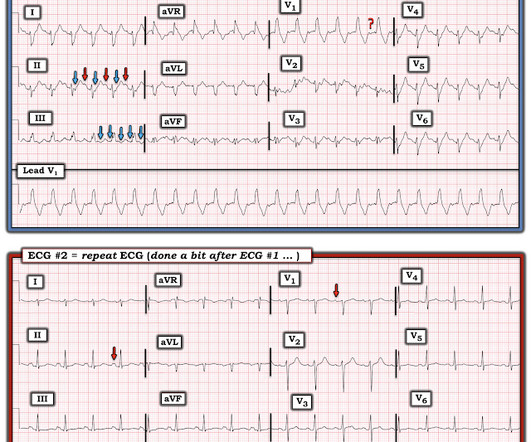
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. Learning Point: 1. As is often emphasized on Dr. Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". The cath lab was activated by the medics.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. At midnight.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
Intensive Care Research , 1 (3-4), pp.60-64. Even though sedation after endotracheal intubation (ETI) reduces the risk of self-extubation, uncontrolled pain, and awakening awareness, several small single-centre studies demonstrate low rates of sedative drug administration after ETI in the emergency department (ED). Epub 2014 Sep 9.
Clinical Question: Does simultaneously performing the modified valsalva maneuver and administering intravenous adenosine, compared to either treatment alone, have greater success in achieving normal sinus rhythm in patients presenting to the ED with PSVT? 2010;17(1):44-49. Duration of Antiarrhythmic Effect: MVM group: 35.44
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
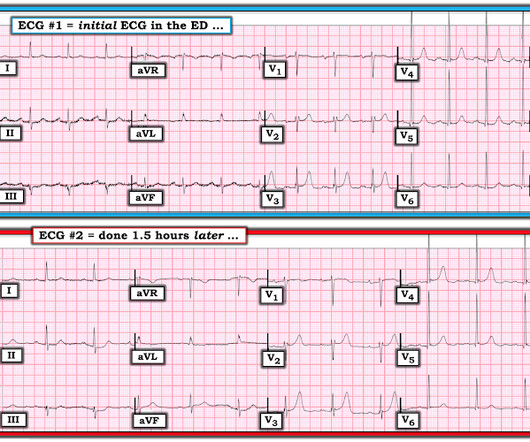
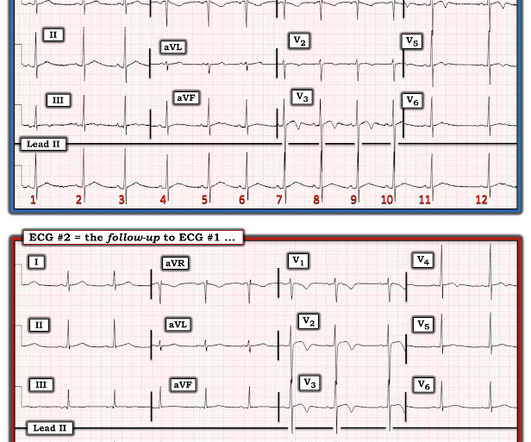
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case. After seeing ECG #2 — Can you explain: i ) Why no negative P wave was seen in lead V1 of ECG #1? —
2024 Oct 9. You can find more details in the full blog post. There were no differences in survival (12% with IO vs 10% with IV) or neurologically intact survival (9% vs 8%). 2024 Nov 1. Restrictive vs Liberal Transfusion Strategy in Patients With Acute Brain Injury: The TRAIN Randomized Clinical Trial. doi: 10.1001/jama.2024.20424.
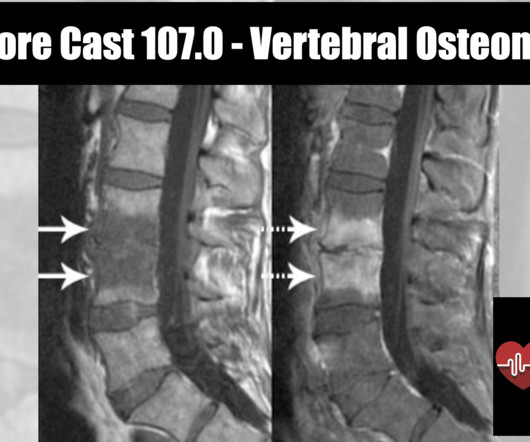
Epidemiology 1 to 2.4 cases per 100,000 people ( Zimmerli 2010 ) More common in males with M:F of 3:1 Rate is also increasing due to increased number of spinal procedures Typically affects adults, with most cases occurring in patients over 50 years old. Other pathogens include: E. Often used interchangeably with osteomyelitis.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. per year incidence of SCD in this cohort [1].
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Figure-1: The initial ECG in today's case — obtained after ROSC.
A 74-year-old female with a past medical history of hypertension, diabetes, recent basilar artery stent placement with a 20 pack-year smoking history presents to the ED via EMS for altered mental status and episodes of apnea. CT head without contrast 1 is performed and reveals the following: Question: What is the diagnosis?
Features Urticaria and pruritis Rapid onset (1-2 hours) IgE Dependent (Type I Hypersensitivity) Reactions An allergen cross-links two or more IgE molecules on mast cells or basophils and initiates a signal cascade leading to degranulation. J Allergy Clin Immune Tract 2017; 5(5): 1402-9. In: UptoDate, Feldweg AM (ed.)
Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED.
[link] Case continued She arrived in the ED and here is the first ED ECG. IMPRESSION: 1. We know that most type 1 acute MI due to plaque rupture and thrombosis occurs in lesions that are less than 50% (see Libby reference). I don't know if her pain was getting better or not. The Queen no longer thinks it is OMI.
Patients were randomized in a 1:1 ratio. Key Secondary Endpoints: 5 (3.9%) patients in the IV cetirizine group returned to any ED or clinic within 24 hours compared to 15 (11.1%) in the IV diphenhydramine group; P=0.04 Risk of first-generation H(1)-antihistamines: a GA(2)LEN position paper. 2005 Sep;116(3):643-9.
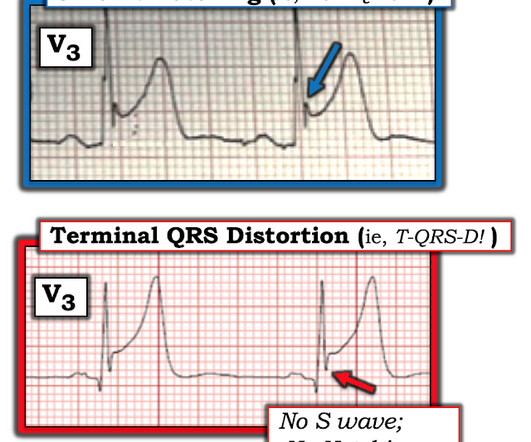
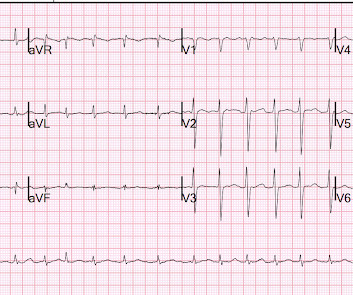
I’ve taken th e l ead V 3 examples in Figure-1 from previous cases posted on Dr. Smith’s ECG Blog : T OP in Figure-1 — Despite marked ST elevation in this lead V3 — this is not T-QRS-D, because there is well-defined J-point notching ( BLUE arrow ). This patient had a repolarization variant as the reason for ST elevation.
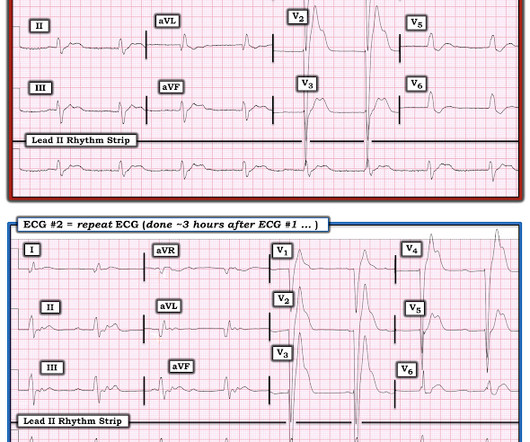
mg/dL (sorry, Europeans, for the weird units) Here was the initial ED ECG: There is a junctional rhythm with retrograde P-waves (see the dip in the T-wave in lead II across the bottom; you can follow that up to all the other leads and see the retrograde P wave). Learning Points: 1. Figure-1: The first 2 tracings in today's case.
He was brought to the ED. To me, it was clearly atrial flutter with 1:1 conduction. Continue Eliquis 5mg BID, should be continued for 3 months == MY Comment , by K EN G RAUER, MD ( 9/18 /2024 ): == I found the following aspects of today's case of special interest. They did not feel they had time to sedate.
Here is his ED ECG: There is bradycardia with a junctional escape. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. He appeared gray in color, with cool skin.
These were read by our fantastic chief of radiology, Gopal Punjabi, who has his own blog on Spectral CT: [link] [link] Here is the image using Spectral CT : It is much more obvious with this technique! For clarity — I’ve put these first 2 tracings together in Figure-1. Figure-1: The first 2 ECGs in this case ( See text ).
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. LEARNING POINT : 1. For clarity in Figure-1 — I've reproduced and put together the 2 serial ECGs that were texted to Dr. Smith in today's case. in ECG #1 ). in ECG #1 ).
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. As we have described multiple times on this blog, false positive "pericarditis" kills by distracting the clinician from actual emergencies including OMI, dissection, PE, and others. 15-9/6/2017 ).
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% per year incidence of SCD in this cohort [1].
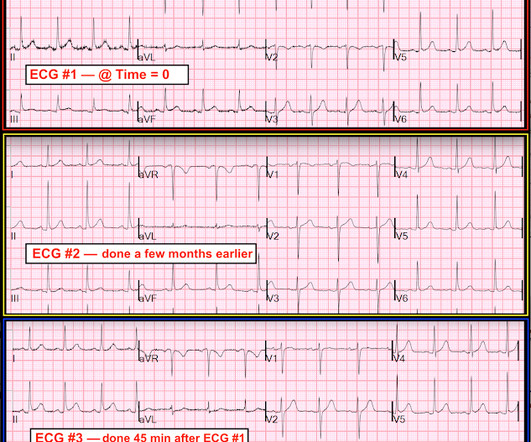
The ED was incredibly busy, with 40 patients waiting in triage for beds (all of whom I had already screened), so we put her in a chair in triage. Figure-1: Comparison of the 3 ECGs in this case ( See text below ). The presence of artifact should be noted in ECG #1. So I was not entirely convinced.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Setting – large, academic, suburban ED. Figure-1: The initial ECG in today's case.
These are reasons why it does not look like OMI: 1. Serial Troponins remained in the 9-11 range, w/o any large rise and/or fall, also atypical for OMI. The patient is a 30-ish year old man, who presented to the ED with a 1-week history of chest pain that was mostly right-sided — and improved with sitting up.
For clarity — I’ve put these 2 tracings together in Figure-1. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). The ECG finding that I KNOW is real in ECG #1 is the mirror - image appearance of ST-T waves in leads III and aVL.
PSA, also referred to as intravenous sedation in this paper, requires considerable resources, including 1:1 nursing observation, and burdens the emergency department (ED). 0.33, I2 = 0, moderate certainty) Mean ED length of stay was signifficantly shorter in the IAL group compared to the PSA group. h; 95% CI − 2.48
Clinical Scenario: A 34-year-old woman presents to the ED with back pain. Schwartz and colleagues performed an ingenious trial ( Schwartz 2000 ) Enrolled 64 ED patients with acute pain. Read More REBEL EM: The Ketorolac Analgesic Ceiling References Irizarry E et al. Can J Emerg Med 2007; 9(1): 30-2.
You, however, are working an ED shift, and when you see the name “Barbie Junior” on your computer screen, your heart does a flutter. It can be in started in the ED, and many of us are already using it. Soon, she was too breathless to feed, and Barbie and Ken were panic-stricken at how pale and lethargic she looked. days compared to 1.50
On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. Another ECG was obtained during pacing: Mostly paced rhythm with PVCs (#3, #6, #9, #12). The ED team again pointed out the evidence of inferoposterior OMI, this time by the modified Sgarbossa criteria. mm STE with 9.5 mm STE with 9.5
This ECG is quite obvious for long-time readers, and you may think this far too easy to be presented on this blog. mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent."
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Then, 1 hour before arrival, it recurred, again lasting 5 minutes. 911 was called and this prehospital ECG was recorded at time zero: Limb leads: Note the artifact that is simultaneously recorded in all limb leads. . == Comment by K EN G RAUER, MD ( 9/22/2019 ): == There are important concepts to emphasize in this case by Dr. Smith.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chest pain and shortness of breath after finishing a 4-mile run. At the time of evaluation in the ED, his symptoms were resolved. He typically runs 4 to 8 miles per day.
Vittinghoff, E. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. The prohibition against beta blockade in cocaine toxicity, causing "unopposed alpha" stimulation, needs to be re-examined. is intuitive, and not surprising.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content