This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
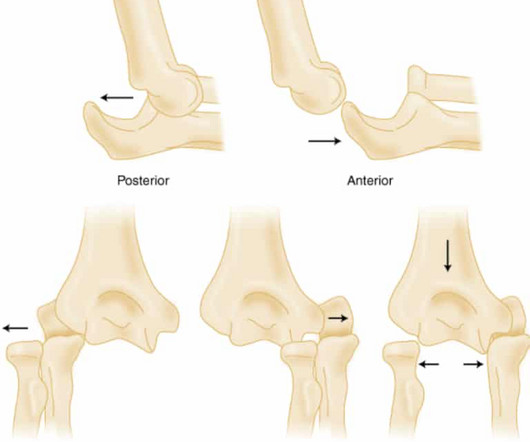
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
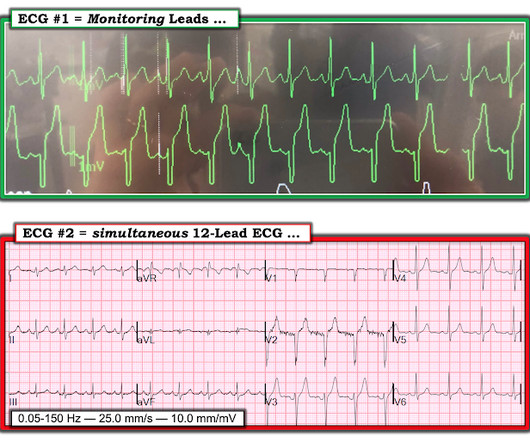
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
No significant differences in heart rate 1 minute after cardioversion were observed between the three groups. What they did: Prospective randomized controlled trial, unblinded, multicenter study Conducted from January 2017 to December 2022 Patients with confirmed PSVT were randomly assigned to receive MVM, IV Adenosine, or combined therapy.
I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I had only 9 false positives but I missed 2 OMI. This was sent to me from Sam Ghali ( @EM_Resus ) with no other information. I assumed it was a patient with acute chest pain. Real or just fake?"
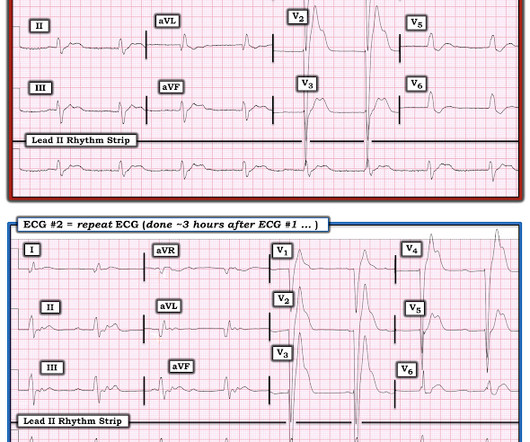
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al.
Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). Answer : Bedside ultrasound!
ECG #1 Interpretation: ECG #1 shows sinus rhythm at a heart rate of 77 bpm. Following more detailed questioning — it turned out the patient had started taking 9 different herbal remedies to ease lethargy and unspecific neurological symptoms. For clarity in Figure-1 — I've reproduced the initial ECG in today's case.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight. At midnight.
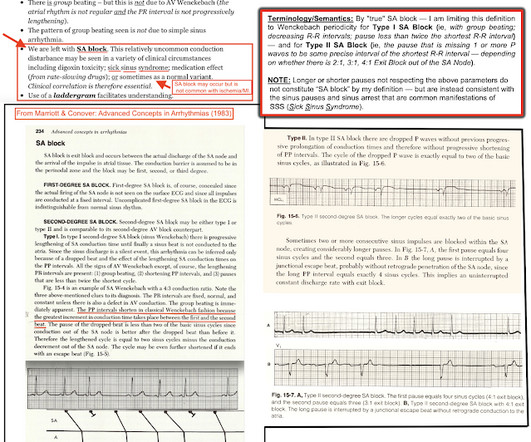
R waves 6 through 9 have no preceding P waves and are suspiciously regularly spaced. Impulses E, F, G, H, and I were blocked. Progress in Biophysics and Molecular Biology , 120 (1–3), 164–178. Science Translational Medicine , 9 (400). Janssen, P. & Fedorov, V. link] Li, N., Hansen, B. Ignozzi, A. Zakharkin, S.
1, 2 Its occurrence often portends worse outcomes in intubated patients, whose projected hospital course was already tenuous. 1, 4, 6 The overall incidence of VAP is somewhere around 5%-40% of all intubated patients, depending on the study and country from which it is reported. 4, 8 Paper: Dahyot-Fizelier, C.,
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
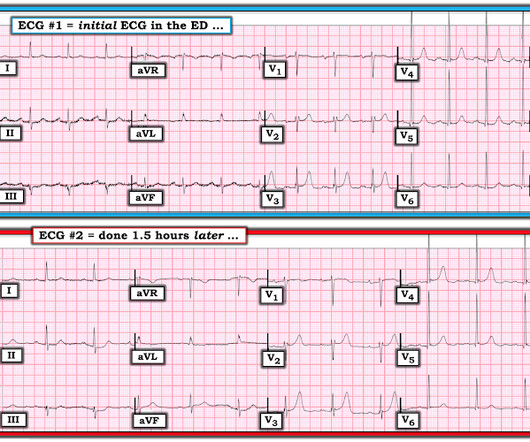
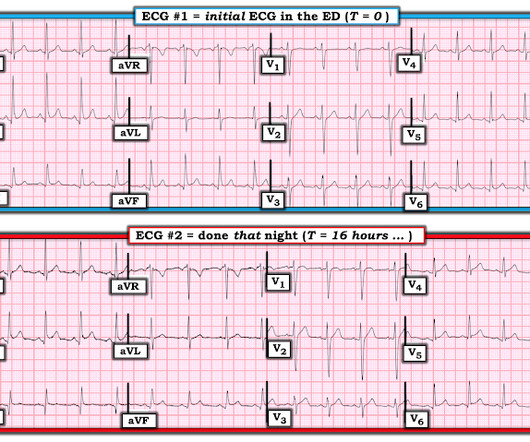
Learning Point: 1. Smith's ECG Blog — the evolution of an acute OMI is not necessarily static — but may be "dynamic". For examples of this phenomenon — See My Comment in the February 14, 2018 — July 21, 2020 — and December 22, 2022 posts in Dr. Smith's ECG Blog ). Figure-1: Comparison between the first 3 ECGs in today's case.
2024 Oct 9. You can find more details in the full blog post. There were no differences in survival (12% with IO vs 10% with IV) or neurologically intact survival (9% vs 8%). There is a bunch more – so have a listen or watch us on Youtube feed below. You can read all the papers on the links in the show notes right here.
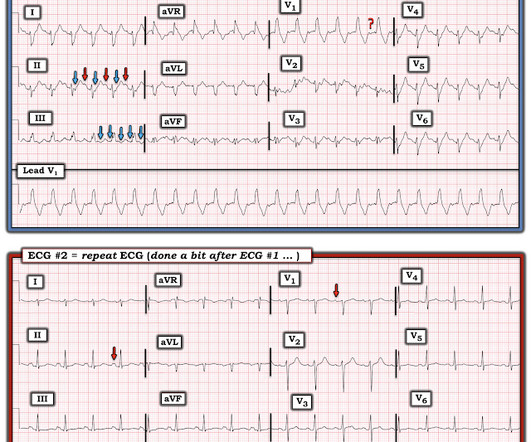
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% He denied chest pain or shortness of breath.
What They Did: Design: Randomized, controlled, blinded-outcome trial Sites: Three emergency departments in Denmark Duration: October 9, 2019 to May 26, 2021. Patients : Compared standard of care to serial US plus stand care in patients with dyspnea. to −0.66) and −1.66 (95% CI −2.09 to −0.78) and -1.97 (95% CI −2.70
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case. After seeing ECG #2 — Can you explain: i ) Why no negative P wave was seen in lead V1 of ECG #1? —
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Guideline-based and restricted fluid resuscitation strategy in sepsis patients with heart failure: A systematic review and meta-analysis [published online ahead of print, 2023 Aug 9]. References: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM.
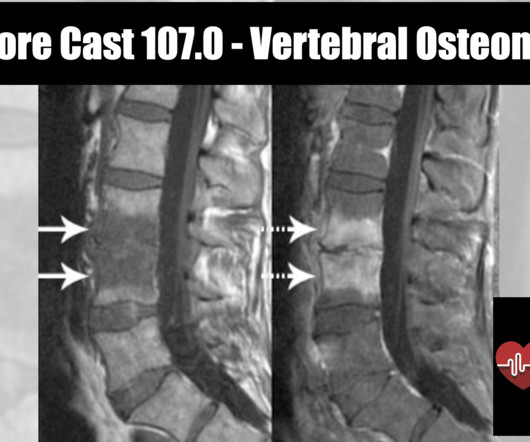
Epidemiology 1 to 2.4 cases per 100,000 people ( Zimmerli 2010 ) More common in males with M:F of 3:1 Rate is also increasing due to increased number of spinal procedures Typically affects adults, with most cases occurring in patients over 50 years old. Other pathogens include: E. Often used interchangeably with osteomyelitis.
Intensive Care Research , 1 (3-4), pp.60-64. This blog, like the paper cited, is dedicated to him. Tragically, several attempts at resuscitation upon arrival at the emergency department were unsuccessful. This article is based on: Mayberry, H., Burgart, A.M. and Kanaris, C., Intubated, awake, and paralysed: a never event.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Figure-1: The initial ECG in today's case — obtained after ROSC.
CT head without contrast 1 is performed and reveals the following: Question: What is the diagnosis? On exam, the patient opens eyes to voice, has extraocular movements intact, is unable to speak, and has 0/5 strength in all extremities. The patient was intubated for acute hypercapnic and hypoxic respiratory failure and airway protection.
Spikes 2, 3, 4, 5, 7, 8, and 9 all occur either during or immediately after P waves which should never happen. He had routine follow up for the mitral valve clip approximately 1 month after the procedure, and the note indicated recognition of atrial lead dislodgement on the CT scan from the hospitalization a few weeks prior.
Features Urticaria and pruritis Rapid onset (1-2 hours) IgE Dependent (Type I Hypersensitivity) Reactions An allergen cross-links two or more IgE molecules on mast cells or basophils and initiates a signal cascade leading to degranulation. of people who take NSAIDs ( Nzeako 2010 ). of people who take NSAIDs ( Nzeako 2010 ).
LBBB also has discordant STE in V1-V3 and STD in V5, 6 -- I will not be giving examples of this, as they are readily available all over the blog. Missed LAD Occlusion with Swirl, peak trop 80 ng/mL (equivalent to 80,000 ng/L), diagnosed as "Non-STEMI" Case 9. As always, LAD OMI need not meet STEMI criteria and usually does NOT!
Despite a plateau in overall union membership of around 10% in 2023 1 , major labor actions shook the U.S. 2023 October 9. 2012 Feb 1;4(1):127-57. Author: Ryan Leone, MSc, Medical Student at Columbia University // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) What’s the issue? Frequency : In the U.S.,
Sites: Investigators recruited patients at 31 French emergency departments at university and nonuniversity hospitals Duration : June 1, 2009 to March 31, 2015. Recurrence of pneumothorax within 1 year. They concluded that more research of higher quality is needed to strengthen the evidence in favor of one technique over the other.
Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED. The primary purpose of Table 1 is to provide a summary of baseline characteristics and demographics of the study population, presenting data in a clear and organized manner.
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT Coronary Angiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. Atropine usually works in junctional rhythm with a narrow complex 9. What is the atrial activity? What to do?
This blog is an example of exactly that. While transporting to the emergency department, the patient’s mother informed me that PDCD affects less than 1 in 50,000 individuals and is more common in males than females. But this would be an impossible expectation, especially in the environment in which we practice medicine.
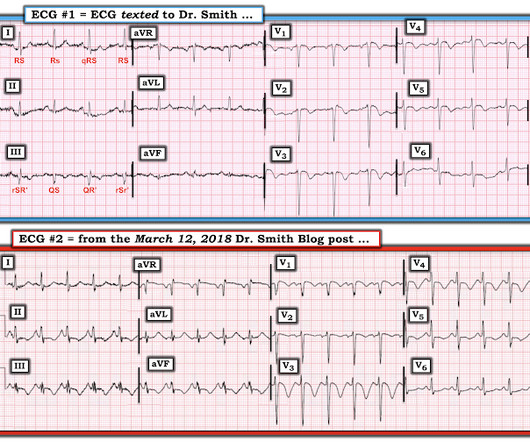
This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. Learning Points: 1. For clarity in Figure-1 — I've reproduced and put these first 2 ECGs together. Figure-1: The first 2 tracings in today's case.
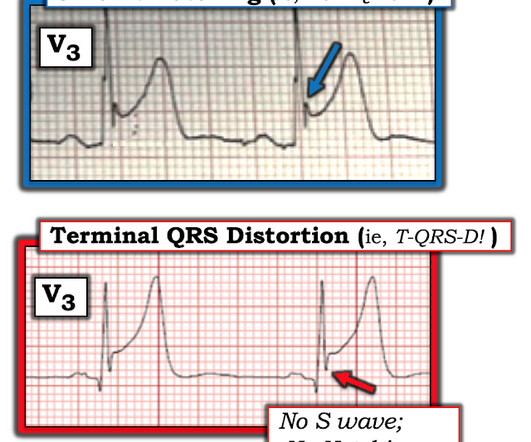
I’ve taken th e l ead V 3 examples in Figure-1 from previous cases posted on Dr. Smith’s ECG Blog : T OP in Figure-1 — Despite marked ST elevation in this lead V3 — this is not T-QRS-D, because there is well-defined J-point notching ( BLUE arrow ). Although simple to define — this finding may be subtle!
To me, it was clearly atrial flutter with 1:1 conduction. Continue Eliquis 5mg BID, should be continued for 3 months == MY Comment , by K EN G RAUER, MD ( 9/18 /2024 ): == I found the following aspects of today's case of special interest. Why did Dr. Smith immediately say the rhythm was AFlutter with 1:1 AV conduction?
Over the last 1 week, her exertional chest pain became worse both in intensity and triggering threshold. She underwent exercise echocardiogram in mid October where she exercised for nearly 7 minutes on the standard Bruce protocol and had typical anginal pain and shortness of breath. But the patient has active chest pain. link] Shvilkin et al.
These were read by our fantastic chief of radiology, Gopal Punjabi, who has his own blog on Spectral CT: [link] [link] Here is the image using Spectral CT : It is much more obvious with this technique! For clarity — I’ve put these first 2 tracings together in Figure-1. Figure-1: The first 2 ECGs in this case ( See text ).
The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chest pain. Today’s case provides perhaps the best example of s erial E CG e volution of this elusive entity.
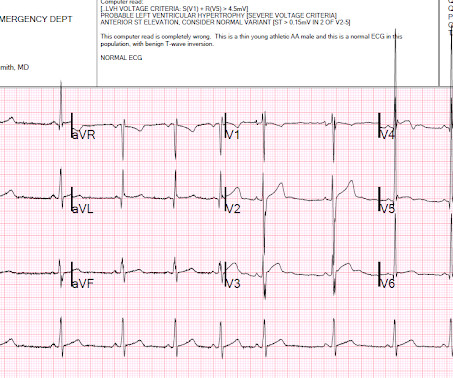
After having learned about benign T wave inversion pattern years ago on this blog, and having seen many cases on this blog and in my practice since then, I instantly recognize this as BTWI, a fairly common normal variant. see below for more info on this) 1. POINT # 2: The E CG F indings C hanged !
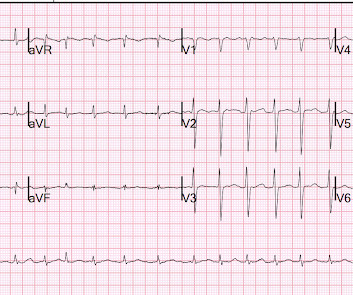
The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% The article is edited by Smith. F (rectal).
Hyperkalemia and ST Segment Elevation, Post 1 A Tragic Case, related to the last post A patient with chest pain and ST Elevation in V1 and V2 You MUST recognize this pattern, even if it is not common ST Elevation. Figure-1: I've reproduced the initial ECG in today's case. Fluid resuscitation was initiated. What is it?
This trial aimed to assess whether targeted therapeutic mild hypercapnia (TTMH) applied during the initial 24 hours of mechanical ventilation in the ICU can enhance neurological outcomes at the 6-month mark, as compared to standard care, which involves targeted normocapnia (TN). Paper: Eastwood G, et al. N Engl J Med. Epub 2023 Jun 15.
4 important features that indicate acute right hear strain: 1. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with APE (p less than 0.001). They found that only 11% of PE had 1 mm T-wave inversions in both lead III and lead V1, vs. 4.6%
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. As we have described multiple times on this blog, false positive "pericarditis" kills by distracting the clinician from actual emergencies including OMI, dissection, PE, and others. 15-9/6/2017 ).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content