This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Fever in the Emergency Department Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. Outside his family and work, Jesse pours […] The post SGEM#195: Some Like It Hot – ED Temperature and ICU Survival first appeared on The Skeptics Guide to Emergency Medicine. Critical Care Medicine 2017.
Historically, it has been used more frequently in the ICU than in Emergency Departments, likely due to provider comfort. […] The post Is there a Precedence for Precedex in the ED? appeared first on EMOttawa Blog.
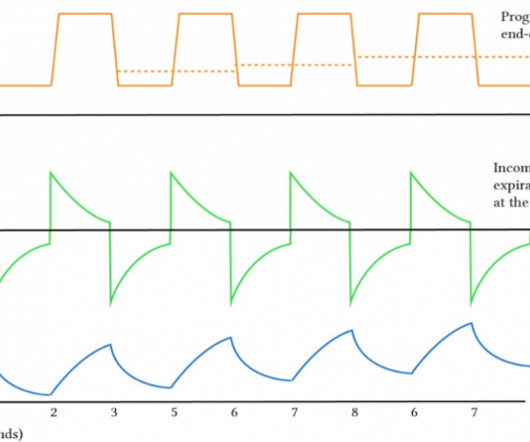
Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. There is certainly a need for more practical application for the ED doc or initial setup of patients on the vent.
Background: Patients with decreased level of consciousness due to alcohol, drugs, or medications commonly present to the ED. PMID: 38019968 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The NICO Trial: NIV in Comatose Patients with Acute Poisoning appeared first on REBEL EM - Emergency Medicine Blog.
Back on June 1 st , 2023, Swami wrote a blog post on REBEL EM titled, The CT FIRST Trial, Should We Pan-CT After ROSC? REBEL EM Blog, June 1, 2023. Back on June 1st, 2023, Swami wrote a blog post on REBEL EM titled, The CT FIRST Trial, Should We Pan-CT After ROSC? Below you will find some of the points we discussed.
REBEL Cast Ep120: Etomidate vs Ketamine for RSI in the ED? PMID: Clinical Question: Does a single dose of ketamine or etomidate used for rapid sequence intubation (RSI) of critically adults in the ED impact the SOFA score within 3 days of hospitalization? appeared first on REBEL EM - Emergency Medicine Blog. 95% CI -1.4
Full blog post here. European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. If you could achieve this process in your ED – then great.
Mild to moderate DKA represents a subgroup of patients that often require admission to the ICU due to hospital policies not allowing insulin infusions outside of this clinical setting. The SQuID Protocol (Subcutaneous Insulin in /diabetic Ketoacidosis): Impacts on ED Operational Metrics. Paper: Griffey RT et al. Acad Emerg Med 2023.
He was intubated on arrival at the ED for mental status and airway protection due to vomiting. His temperature was brought back to normal over time in the ICU. See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 There is also large T wave inversion and long QT.
Salim is also the creator and founder of REBEL EM and REBEL Cast, a free, critical appraisal blog and podcast that try to cut down knowledge translation gaps of research to bedside clinical practice. Case: A 59-year-old woman presents to the emergency department (ED) with fever, tachycardia, and hypotension.
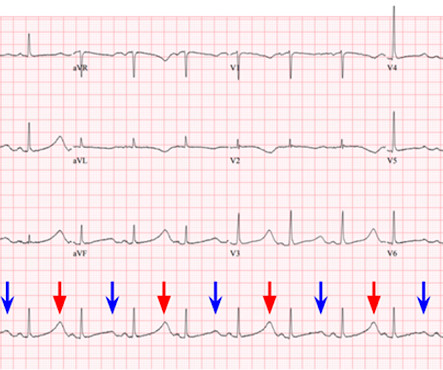
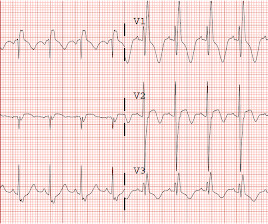
On arrival to the ED the patient was intubated with normal vital signs. She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes. What is ELECTRICAL ALTERNANS?
They consecutively enrolled 1,817 ICU patients from 45 sites across China. Population: Inclusion Criteria: Age 18-75 years old SOFA score 2-13 Admitted to the ICU with a diagnosis of sepsis 3.0, “ Life-threatening organ dysfunction caused by a dysregulated host response to infection.” 002) ICU-free days: Placebo 12.4%
In our first part, we talked about the basics of mechanical ventilation and how to set up the ventilator for the busy ED doc! If you haven’t read part one – check it out here! […] The post Lung Protective Ventilation appeared first on EMOttawa Blog.
The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. This patient presented to the ED “after a couple of days of chest discomfort”. I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!)
2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Over the past few years, there has been an increase in emergency department (ED) volumes and lengths of stay. The typical nursing to patient ratio is 1:3 with a shared respiratory therapist for the entire ED.
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. I interpreted this tracing knowing only that the patient was a woman in her 60s, with a prior history of proximal LAD OMI — who now presented to the ED with a history of new chest discomfort and shortness of breath.
Bottom Line Up Top: In patients with infectious processes that are stable for discharge home, there is no role for giving a first dose of antibiotics IV in the ED. BMJ (Clinical research ed.). Factors influencing the development of antibiotic associated diarrhea in ED patients discharged home: risk of administering IV antibiotics.
The patient was upgraded to the ICU for closer monitoring. The RR ( R espiratory R ate ) in today's case is recorded as 14/minute at the time the patient presented to the ED on the day after their initial presentation. Echocardiogram showed severe RV dilation with McConnell’s sign and an elevated RVSP.
The patient was admitted to the ICU for close monitoring and electrolyte repletion and had an uneventful hospital course. The patient is a man in his 60s with established severe alcohol use disorder — and epidural abscess being treated with longterm Ciprofloxacin — who presented to the ED following a syncopal episode. As per Drs.
This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so. The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. J Med Toxicol. Epub 2019 Jul 3. PMID: 31270748 Maheshwari K, et al. Am J Emerg Med.
A patient had 3rd degree AV block in the ED. Nevertheless, clinicians involved in emergency care will periodically encounter pacemaker issues — which underscores the importance of today's blog post. and the 2021 YouTube Review by ICU Advantage on "Temporary Pacemakers: Modes and Basic Settings".
Patients were started on low-dose norepinephrine at a median time from ED arrival of 93 minutes compared to 192minutes in the standard care arm. The goal of the trial was to see if early vasopressors improved shock control by 6 hours. This resulted in better shock control by 6hrs (76.1% Liberal: 14.9% Estimated Difference: -0.9%; 95% CI 04.4
Case A young man was brought to the ED by friends with a complaint of progressive weakness to the point of extremity paralysis on arrival. The patient was admitted to the ICU. The potassium was repleted in the ICU to a total of 170 mEq with resolution of symptoms (this could be hazardous!). The K returned at 1.4
mg/dL (sorry, Europeans, for the weird units) Here was the initial ED ECG: There is a junctional rhythm with retrograde P-waves (see the dip in the T-wave in lead II across the bottom; you can follow that up to all the other leads and see the retrograde P wave). He was admitted to the ICU and was unstable, in shock, overnight.
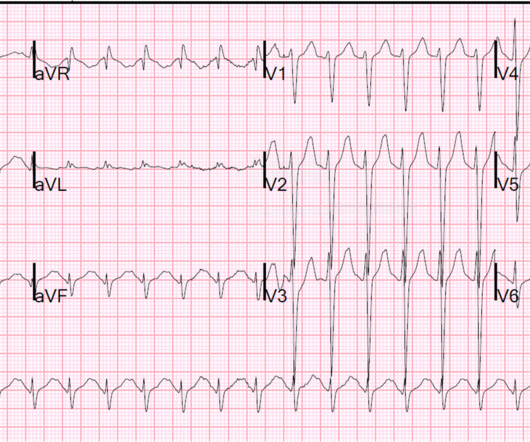
Adapted from Dr. Smith’s EKG Blog. Source: [link] As you are calling the ICU and cardiology team, the patient has recurrence of her symptoms and repeat ECG shows return of the PVT. A simplified standard protocol for ED management is below 3. An ECG is performed and is shown below: Figure 1. She denies chest pain.
The patient was restless, agitated, and nonverbal on arrival to ED, with elevated HR at 150. Here is the first ED ECG: What is the likely diagnosis? He had a prolonged stay in the ICU requiring days of bicarbonate. His HR was 160 on arrival of EMS, and they gave him adenosine 6 mg and 12 mg and 500 cc NS, but with no response.
In this post, we critically appraise the first systematic review and meta-analysis to compare the safety and efficacy of etomidate and ketamine as induction agents for RSI in the ED and prehospital setting. Pooled data from ED and prehospital were evaluated using an odds ratio with a 95% confidence interval. Article: Sharda SC et al.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). 2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU).
You, however, are working an ED shift, and when you see the name “Barbie Junior” on your computer screen, your heart does a flutter. It can be in started in the ED, and many of us are already using it. Secondary outcome analysis showed there was no difference in length of hospital stay, ICU stay, or duration of oxygen therapy.
3.6 – 55.6) (-) LR: 0.13 (0.08 – 0.20) ED US (+) LR: 9.5 (2.1 3.6 – 55.6) (-) LR: 0.13 (0.08 – 0.20) ED US (+) LR: 9.5 (2.1 ED US 97%% 90%% 9.5 Rezaie, MD (Twitter: @srrezaie ) The post REBEL Core Cast 94.0 – SBO appeared first on REBEL EM - Emergency Medicine Blog. Louis, Mosby, Inc.,
He ended up requiring a total of 13 grams of CaCl in the ED to maintain rhythm and hemodynamics until our dialysis colleagues could start dialysis in the ED. He made it to the ICU, however the patient unfortunately expired approximately 24 hours after ICU admission. These patients cannot afford a delay.
in the ICU but survived with excellent function. As we have described multiple times on this blog, false positive "pericarditis" kills by distracting the clinician from actual emergencies including OMI, dissection, PE, and others. I completely agree with many of the KEY findings conveyed by Dr. Meyers.
95% Confidence Interval) Strengths: The study addresses a patient-centered clinical question that is relevant to ED practice. appeared first on REBEL EM - Emergency Medicine Blog. 2,230 records remained after the elimination of duplicates. 2,210 records were excluded after screening. in ICC group, 5.8%
Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. In the ED, ultrasound showed hemopericardium with tamponade. An ED thoracotomy was done and the pericardium drained and internal compressions continued.
Duration of mechanical ventilation, ICU, and percentage of vasopressor use were not significantly different. All intubations were performed on hospitalized patients, limiting application to the ED population. Day 28 survival rates for both ketamine and etomidate were not significantly different.
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. EMCrit blog website. 6 Position the patient with the head of the bed at 30 to 45 degrees during intubation whenever possible, and use an 8.5 A special thanks to Drs. J Emerg Med. 2017;52(4):433-437.
An example using a real case I had while on call in the ICU: A 61-year-old female had a post-induction arrest on the wards/hospital telemetry floor after being intubated for airway protection. In a PCAC 1 or 2, we may prioritize a cath and tolerate a couple hours without ICU Neuroresuscitation. Great question!
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. On arrival in the ED, he was hypotensive with a systolic blood pressure in the 70s. 72; Issue 9; 2018.
The patient vomited once and given the more intense pain decided to come to the ED. 2-hour hsTn: 615 ng/L; bedside ED echo (without contrast) did not show a clear wall motion abnormality (WMA). Tonight’s episode did not improve with simethicone and Tums as it had previously. No history of GIB, dysuria, or GU symptoms. Abstract 556.
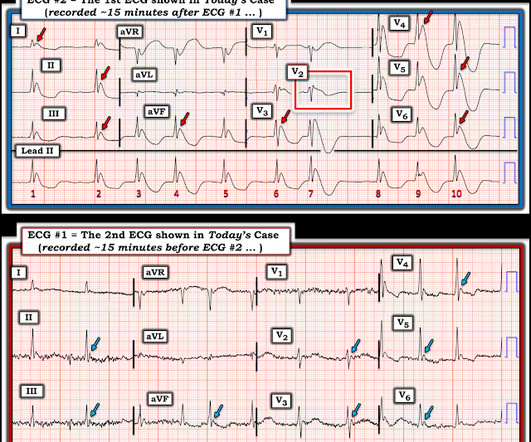
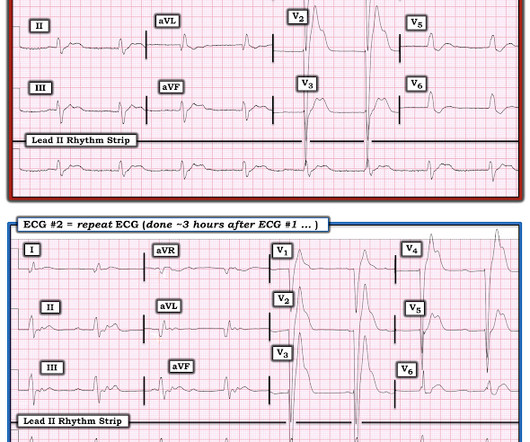
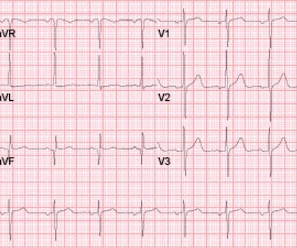
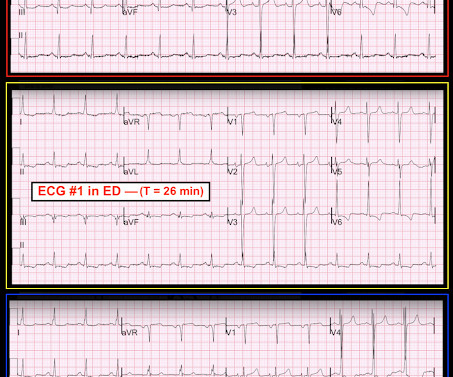
The patient was managed in the ICU and had serial troponins. Figure-1: The first 2 ECGs shown in this case ( See text ). == C OMMENT : As per Dr. Smith — E CG # 1 was the initial tracing on this patient who presented to the ED already intubated for respiratory failure. It is not yet available, but this is your way to get on the list.
Upon arrival in the ICU, before getting Continuous Veno-Venous Hemodialysis (CVVHD), his potassium had risen again to 7.8 Bottom Line: Hyperkalemia is an increasingly common ED diagnosis that must not be missed. At that time his diastolic blood pressure was also hovering between 45 and 55 mmHg.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. Fortunately, he was extubated several days later in the ICU with intact baseline mental status and was discharged shortly thereafter to subacute rehab.
We obtained access and monitoring, but she showed no signs of improvement, and we judged that an intervention must be done in the ED without delay. A CT was obtained later and showed appropriate positioning of the catheter: She was admitted to the ICU and the catheter was used several times to withdraw more fluid.
She was asymptomatic at the time of this ECG recorded on arrival to our ED: What do you think? If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content