This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
As medical education podcasts, videos, and blogs continue to grow in popularity it is crucial that we cite them correctly, both in publications and on our CVs. This blog post provides an update to our 2018 blog articles to reflect these changes. Blogs Last Name First Initial. Blog Title blog. Video Title.
TCP in the ROSC Patient: False Electrical Capture at 75mA Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the second installment of a blog series showing how transcutaneous pacing (TCP) can be difficult and how you can improve your skills. Pacing was continued in the ED, with identical settings.
The AVAPS mode is as effective and safe as BPAP S/T in treating patients with hypercapnic respiratory failure in the ED.” Clinical Take Home Point: I n patients presenting to the ED with hypercapnic respiratory failure, AVAPS did lead to a faster improvement in pH and PaCO2 levels compared to BPAP S/T. AVAPS: 0.07 AVAPS: 10.20
DISCLAIMER: THE VIEWS AND OPINIONS OF THIS BLOG AND PODCAST DO NOT REPRESENT THE UNITED STATES GOVERNMENT OR THE US MILITARY. Case: A 24-year-old manual labourer presents to the emergency department (ED) after drinking a few too many beers, having a disagreement with another beer drinker and gets knocked down.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." It relies on an 1 mm cut point, which this blog does not favor as an approach to ECG. Smith comment: But the tests (ECG and troponin) are extremely specific and so the post test probability is nearly 100%.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chest pain around 1500 while eating. Patient 2 , EKG 1: What do you think? The patient had none of these conditions.
Clinical Question: Does simultaneously performing the modified valsalva maneuver and administering intravenous adenosine, compared to either treatment alone, have greater success in achieving normal sinus rhythm in patients presenting to the ED with PSVT? This absence of detail leaves the study open to bias.
He currently practices emergency medicine in New Mexico in the ED, in the field with EMS and with the UNM Lifeguard Air Emergency Services. Background: We’ve discussed out-of-hospital cardiac arrest (OHCA) at least once or twice on the SGEM (see long list at end of blog). Your partner asks if you want to administer naloxone as well.
8 blog posts met our standard of online excellence and were approved for residency training by the AIR Series Board. Digital Impact Factor: A Quality Index for Educational Blogs and Podcasts in Emergency Medicine and Critical Care. More specifically, we identified 3 AIR and 5 Honorable Mentions. Please go to the above link.
Full blog post here. European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. If you could achieve this process in your ED – then great.
In many emergency departments (ED), US machines are readily available and can be used to rapidly assess and monitor patients with acute dyspnea at the bedside. US, compared with CXR and CT, offers the absence of ionizing radiation and high reproducibility. Emerg Med J. 2023;40(10):700-707.
6 blog posts met our standard of online excellence and were approved for residency training by the AIR Series Board. More specifically, we identified 2 AIR and 4 Honorable Mentions. These posts have been flagged by and agreed upon by AIR Board members as worthwhile, accurate, unbiased, and appropriately referenced despite an average score.
Here is the prehospital ECG: First ED ECG What do you think? Here is the prehospital ECG: First ED ECG What do you think? He states that he maybe missed a dose or two during recent illness. On EMS arrival, patient's oxygen saturation was in the high 80s and improved on 4L O2 via nasal cannula. SVT with aberrancy?
Urine drug (or toxicologic) screens are a fairly standard tool used in addictions, psychiatry and the Emergency Department (ED), often employed to detect substance use in patients presenting with altered mental status, trauma, psychiatric or abnormal behaviour.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
There is certainly a need for more practical application for the ED doc or initial setup of patients on the vent. With both ER and ICU experience, this post acts as a quick […] The post Mechanical Ventilation Basics appeared first on EMOttawa Blog.
Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. On ED arrival ROSC is achieved. They are unable to feel a pulse and resume CPR.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
6 blog posts met our standard of online excellence and were approved for residency training by the AIR Series Board. Digital Impact Factor: A Quality Index for Educational Blogs and Podcasts in Emergency Medicine and Critical Care. More specifically, we identified 3 AIR and 3 Honorable Mentions. Please go to the above link.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" On arrival to the ED, while waiting for cath lab team, he obtained another ECG: You can now see the full voltage of the high-voltage QRS, likely with some degree of LVH. Both were awake and alert with normal vital signs.
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
REBEL Cast Ep120: Etomidate vs Ketamine for RSI in the ED? PMID: Clinical Question: Does a single dose of ketamine or etomidate used for rapid sequence intubation (RSI) of critically adults in the ED impact the SOFA score within 3 days of hospitalization? Click here for Direct Download of the Podcast Paper: Knack SKS et al.
He called EMS who brought him to the ED. ED Diagnoses: 1. The basic principles of emergency ECG interpretation in patients who present to an ED with new symptoms include the following: Respect the History. He had active chest pain at the time of triage at 0137 at night, with this triage ECG: What do you think? Epigastric pain 2.
Back on June 1 st , 2023, Swami wrote a blog post on REBEL EM titled, The CT FIRST Trial, Should We Pan-CT After ROSC? REBEL EM Blog, June 1, 2023. Back on June 1st, 2023, Swami wrote a blog post on REBEL EM titled, The CT FIRST Trial, Should We Pan-CT After ROSC? Below you will find some of the points we discussed.
These statistics make the ED a crucial treatment initiation point to prevent further morbidity and mortality from opioid overdoses. The benefit of accessibility, availability, and safety of buprenorphine compared to methadone makes it a viable option for opioid use disorder treatment initiation in the ED. PMID 33392580.
Chris also has his own #FOAMed blog called Standing on the Corner Minding My Own Business ( SOCMOB ). Case: A 54-year-old female presents to the emergency department (ED) with abdominal pain and profuse non-bloody diarrhea for the past 24 hours. Her vital signs are within normal limits and she is tolerating oral fluids. AEM Aug 2018.
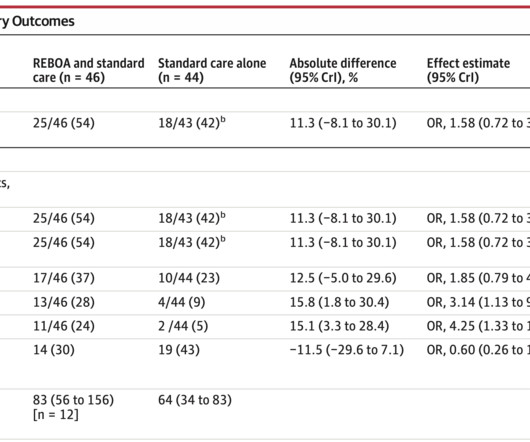
Early expeditious definitive hemorrhage control is a major focus in trauma resuscitation. Patients with torso hemorrhage present a clinical conundrum often requiring interventional radiology or surgery, both of which take time to mobilize. 2 Despite these recommendations there are no randomized clinical trials to help guide practice until now.
He has a wonderful #FOAMed blog and podcast called Broomedocs and also work […] The post SGEM#326: The SALSA Study: Hypertonic Saline to Treat Hyponatremia first appeared on The Skeptics Guide to Emergency Medicine. He has a wonderful #FOAMed blog and podcast called Broomedocs and also work with me on the Primary Care RAP team.
I interpreted this tracing knowing only that the patient was a woman in her 60s, with a prior history of proximal LAD OMI — who now presented to the ED with a history of new chest discomfort and shortness of breath. For more on Precordial Swirl — See the October 15, 2022 post in Dr. Smith's ECG Blog ).
She has contributed to the Academic Life in Emergency Medicine and EM PharmD blogs, […] The post SGEM#203: Let Me Clear My Sore Throat with a Corticosteroid first appeared on The Skeptics Guide to Emergency Medicine. She has contributed to the Academic Life in Emergency Medicine and EM PharmD blogs, and is a part of the ALiEM Capsules Team.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." The ED physicians ECG interpretation of her first ECG was ST elevation in II-aVF and V5-V6,()concave, no reciprocal changes. See > 50 cases on Dr. Smiths EGC Blog.
He is an ED intensivist from New York City and runs the popular EMCrit blog and podcast. He is an ED intensivist from New York City and runs the popular EMCrit blog and podcast. Date: April 10th, 2019 Guest Skeptic: Dr. Scott Weingart. Scott is attempting to bring upstairs care, downstairs one podcast at a time.
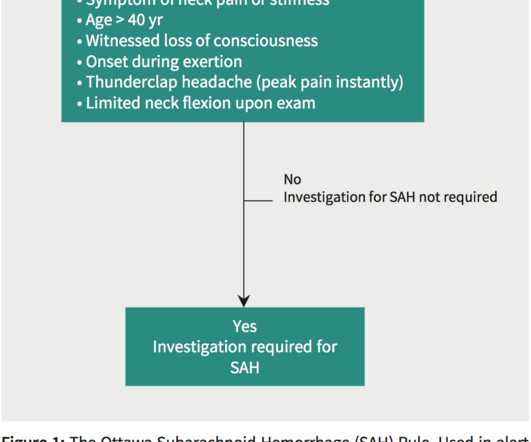
He also has this amazing #FOAMed blog called EM Nerd. He also has this amazing #FOAMed blog called EM Nerd. Population: Neurologically intact adult presenting to the ED with a chief complaint of a nontraumatic, acute headache, or syncope associated with a headache. first appeared on The Skeptics Guide to Emergency Medicine.
He was intubated on arrival at the ED for mental status and airway protection due to vomiting. See our other blog posts of hypothermia and Osborn waves -- Massive Osborn Waves of Severe Hypothermia (23.6 There is also large T wave inversion and long QT. Initial vitals included heart rate 109 bpm and BP 145/92 mmHg.
DISCLAIMER: THE VIEWS AND OPINIONS OF THIS BLOG AND PODCAST DO NOT REPRESENT THE UNITED STATES GOVERNMENT OR THE US MILITARY. DISCLAIMER: THE VIEWS AND OPINIONS OF THIS BLOG AND PODCAST DO NOT REPRESENT THE UNITED STATES GOVERNMENT OR THE US MILITARY. Date: November 30th, 2022 Reference: Johnson et al.
Emlyn’s blog and podcast. Emlyn’s blog and podcast. The bottom line from that episode on skin glue for peripheral intravenous lines was: “Skin glue does appear to decrease the failure rate of IVs in patients admitted to hospital from the ED at 48 hours.
Algorithm: Marquette 12 SL (GE) The Queen gets it right Case 9 (prehospital and ED ECGs). The Queen gets it right First ED ECG: Hyperacute T-waves persist. I have often written about how an ECG interpreted as "normal" by a conventional algorithm may well be manifesting OMI, or even long QT or hyperkalemia. 2 cases at once!
A 56 year old male with PMHx significant for hypertension had chest pain for several hours, then presented to the ED in the middle of the night. He reported chest pain that developed several hours prior to arrival and was 5/10 in intensity. The pain was located in the mid to left chest and developed after riding his bike.
Background: Patients with decreased level of consciousness due to alcohol, drugs, or medications commonly present to the ED. PMID: 38019968 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The NICO Trial: NIV in Comatose Patients with Acute Poisoning appeared first on REBEL EM - Emergency Medicine Blog.
By Sofiya Diurba MD, reviewed by Meyers, Grauer A woman in her 50s with PMH known RBBB and prior syncopal events presents to the ED for five syncopal events over the last 24 hours. This is her first ECG in the ED: What do you see? See these blog posts. Vital signs were within normal limits at the time of triage.
Even though sedation after endotracheal intubation (ETI) reduces the risk of self-extubation, uncontrolled pain, and awakening awareness, several small single-centre studies demonstrate low rates of sedative drug administration after ETI in the emergency department (ED). What are the only exceptions? How can we prevent this?
While statistical likelihood of acute OMI is clearly lower in younger adults — nothing is ruled out by age alone ( as per My Comment in the January 9, 2023 and December 5, 2023 posts in Dr. Smith's ECG Blog ). This was sent to me from Sam Ghali ( @EM_Resus ) with no other information. I assumed it was a patient with acute chest pain.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. Background: Point of care ultrasound (POCUS) has a demonstrated sensitivity of 89.8% and specificity of 88.0%
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content