
ECG Cases 49 – ECG and POCUS for Dyspnea and Chest Pain
Emergency Medicine Cases
APRIL 2, 2024
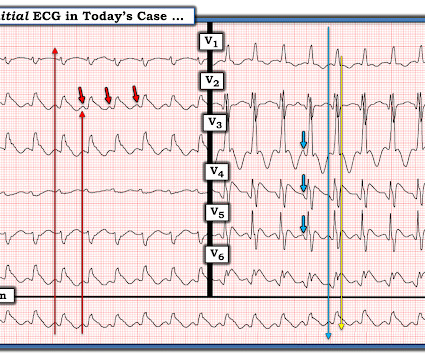
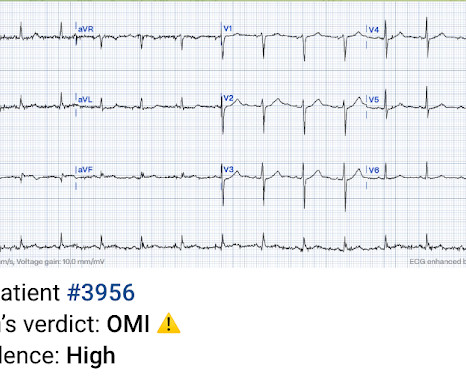
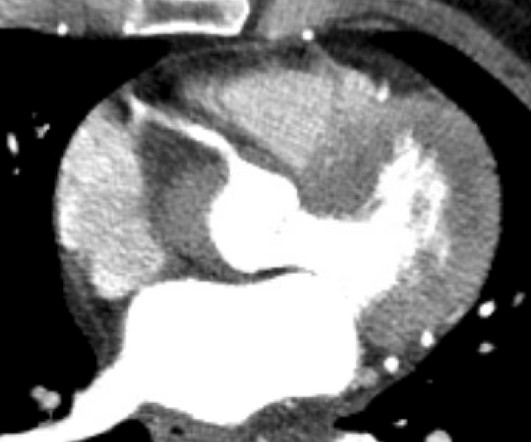
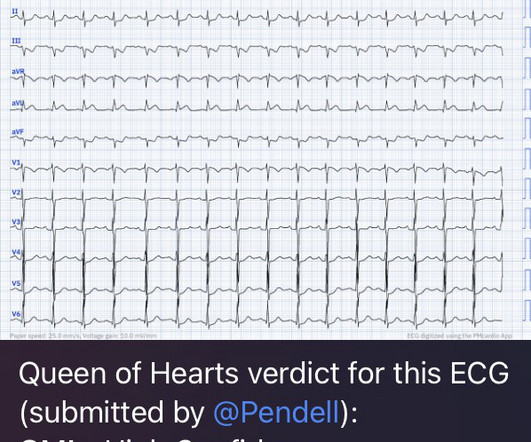
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chest pain. The post ECG Cases 49 – ECG and POCUS for Dyspnea and Chest Pain appeared first on Emergency Medicine Cases.




































Let's personalize your content