This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
By Smith, peer-reviewed by Interventional Cardiologist Emre Aslanger Submitted by anonymous A 53 y.o. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am.
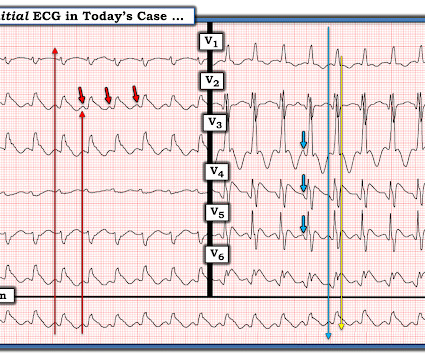
I published, and Emre Aslanger externally validated, the 4-Variable formula for differentiating the ST Elevation of LAD OMI from Normal ST Elevation. Let's stretch out the QRS vertically so it is not so tiny: On upper left is the original. On the right are the precordial leads stretched vertically, so that the QRS is not tiny.
They utilized EMR to gather comprehensive data on patients who received IV calcium and IV diltiazem, or IV diltiazem monotherapy for the treatment of patients with AF/AFL with RVR. The study was dependent on EMR documentation which is prone to error. Hypotension in these patients can complicate management.
This was contributed by Co-editor Emre Aslanger, an interventional cardiologist in Turkey. See My Comment at the bottom of the page in the May 19, 2020 post in Dr. Smith's Blog ). AslangerE A 65-year-old gentleman presented to the emergency department after experiencing two recent ICD shocks in the preceding hours.
History of liver disease, history of substance abuse disorder, and history of delirium tremens were also extracted from the hospital EMR. Background: The emergency department is frequently visited by patients suffering from symptomatic alcohol withdrawal, and the traditional management has been dominated by repeated doses of benzodiazepines.
Written by Emre Aslanger. Emre is a new Editor of the Blog. You can find many examples on this blog attesting that. I am sure that it is not for the readers of this blog. This is also a clear ECG for the readers of this blog, but may be hard for someone who is not used to seeing non-mainstream ECGs.
Epinephrine – 10ug/mL, 10mL syringe Phenylephrine – 100ug/mL, 10mL syringe Phenylephrine bolus doses from 100-200ug and epinephrine 10-20ug administered every 2-5 minutes pursuant to provider order Inclusion Criteria: Adults age >18 years old Received at least one bolus dose of phenylephrine or epinephrine pre-filled syringes Exclusion (..)
In the hope of dispelling continued dependence on millimeter-based STEMI criteria — we’ve published numerous cases in recent years in Dr. Smith’s ECG Blog of acute OMI ( O cclusion-based M yocardial I nfarction ) , in which patients have benefited from acute reperfusion despite not satisfying “STEMI criteria”.
Many researchers, including the editors of this blog, tried to develop such tools in the recent past and we have recommended their use in certain clinical scenarios in many posts on this blog. Smith and Emre Aslanger, but we also thank external researchers for their demonstrative ECGs (thanks to Philip L.
by Emre Aslanger Dr. Aslanger is our newest editorial member. Dr. Aslanger is also the author of the DIFFOCULT study: Emre K. He is an interventional cardiologist in Turkey. Aslanger , a, ⁎ Özlem Yıldırımtürk , b Barış Şimşek , c Emrah Bozbeyoğlu , c Mustafa Aytek Şimşek , a Can Yücel Karabay , b Stephen W. Again nothing diagnostic.
National Registry Certification examinations evaluate the competence of EMS practitioners at a variety of levels, including Emergency Medical Responder (EMR), Emergency Medical Technician (EMT), Advanced Emergency Medical Technician (AEMT), and Paramedic. If that’s the case, please feel free to call our office for additional support.
Reason for intubation, severity of illness, ARDS risk score, and ventilator settings were extracted from the electronic medical record (EMR). Data was automatically captured in the EMR so that accurate information was able to be extracted for the study. of patients left the ED on TV settings of 450 mL and 36.1%
Written by Emre Aslanger (Emre is our newest editor. He is an interventionalist in Turkey and one of 3 originators of the OMI/NOMI paradigm, along with Pendell and Smith. Here are his publications.) Case A 39-year-old male without prior medical history presents with chest pain that started 2 hours prior to presentation. References: 1.
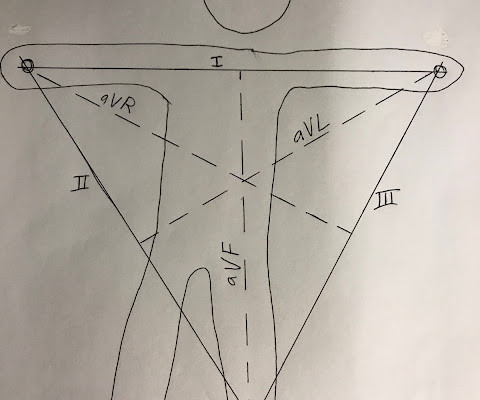
Arterial pulse tapping artifact [link] This online article references the article below by Emre Aslanger, a great guy who occasionally corresponds with me about ECGs. The Wilson (or Goldberger) Central Terminal is used to produce the augmented (a) leads: aVR, aVL, aVF. Aslanger E, Yalin K. Journal of Electrocardiology. 2012;45(1):15-17.
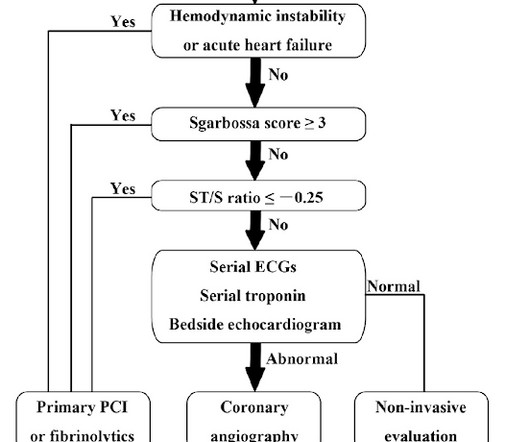
Accordingly, in the algorithm by Cai et al for patients with LBBB and ischemic symptoms ( See below ) — the first indication for PCI is clinical: patients with hemodynamic instability or acute heart failure. An initial level of 650 ng/L represents a too rapid rise to be attributable only to Type II MI from brief cardiac arrest. Learning points 1.
Patient Registry | FHIR Integration Now officially in the Epic Showroom, the Patient Registry FHIR integration improves your data abstraction efficiency by importing data from the hospital EMR system directly into a patient encounter record in the registry. We have even more exciting enhancements in the works for Q3 2024.
V1 has 0.5 mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 mm of elevation. More notably there are hyperacute T waves in V3 through V5. These T waves are too large in proportion to their QRS complexes with broad bases, and they are symmetric or nearly symmetric in appearance.
So under the OMI paradigm, expert-trained AI would help providers identify OMI and this patient would have had immediate cath lab activation, without any need to wait for repeat ECGs or troponin levels. The troponin element is at least one troponin above the 99th percentile URL with rise and/or fall.
Arterial pulse tapping artifact [link] This online article references the article below by Emre Aslanger, a great guy who occasionally corresponds with me about ECGs. The Wilson (or Goldberger) Central Terminal is used to produce the augmented (a) leads: aVR, aVL, aVF. Aslanger E, Yalin K. Journal of Electrocardiology. 2012;45(1):15-17.
An EMR performs emergency medical interventions with minimal equipment. An EMR performs emergency medical interventions with minimal equipment. In this article, we’ll be discussing the differences between a civilian paramedic and a United States Army combat medic. Is this field for me?” or “would I be any good this?”
Reliance on a billing dataset, instead of EMR or prospective data, likely affected the quality of outcome measurement. The heterogeneity of treatment effects was also assessed among different hemoglobin SS genotypes, levels of care, volumes of fluid resuscitation, and diagnosis of acute kidney dysfunction on admission.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content