This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
by Emre Aslanger Dr. Aslanger is our newest editorial member. Dr. Aslanger is also the author of the DIFFOCULT study: Emre K. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. He is an interventional cardiologist in Turkey. Here is the post-intervention angiogram and post-PCI ECG. Turk Kardiyol Dern Ars.
By Smith, peer-reviewed by Interventional Cardiologist Emre Aslanger Submitted by anonymous A 53 y.o. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ). The pain radiated to both shoulders.
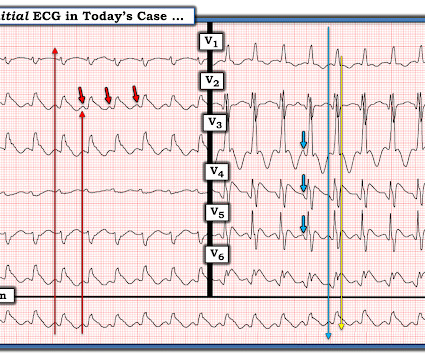
I published, and Emre Aslanger externally validated, the 4-Variable formula for differentiating the ST Elevation of LAD OMI from Normal ST Elevation. Let's stretch out the QRS vertically so it is not so tiny: On upper left is the original. On the right are the precordial leads stretched vertically, so that the QRS is not tiny.
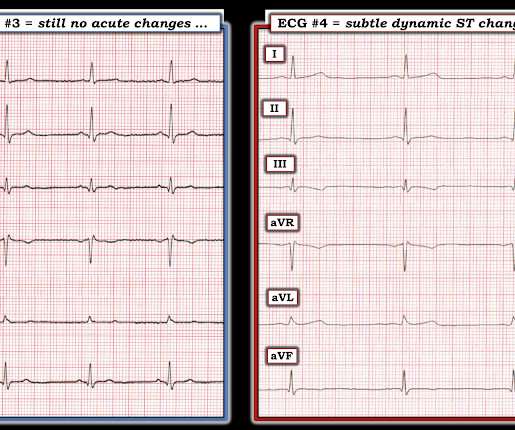
This was contributed by Co-editor Emre Aslanger, an interventional cardiologist in Turkey. As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. That was also my initial concern.
Furthermore, some ECGs may not meet the STEMI criteria but may still be diagnostic for acute coronary occlusion (ACO). Many researchers, including the editors of this blog, tried to develop such tools in the recent past and we have recommended their use in certain clinical scenarios in many posts on this blog.
Written by Emre Aslanger. Emre is a new Editor of the Blog. You can find many examples on this blog attesting that. I am sure that it is not for the readers of this blog. This is also a clear ECG for the readers of this blog, but may be hard for someone who is not used to seeing non-mainstream ECGs.
Now let’s compare this with the existing paradigm to identify multiple preventable delays to reperfusion, which can be improved through the paradigm shift from STEMI to OMI. In the STEMI paradigm, patients with ischemic symptoms and ECGs that don’t meet STEMI criteria get serial ECGs.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
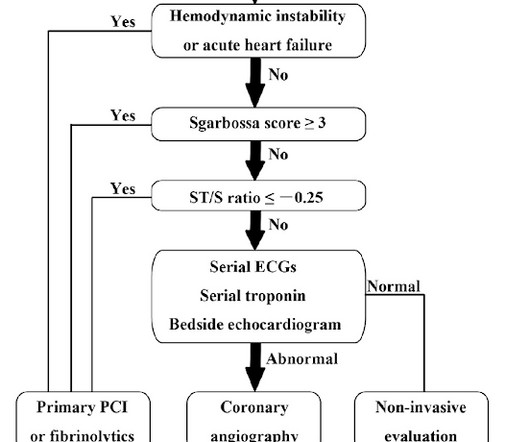
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. On arrival, GCS was 13 and the patient complained of ongoing chest pain.
Written by Emre Aslanger (Emre is our newest editor. More than this — posterior leads that fail to show ST elevation may provide false reassurance ( Please see My Comment at the bottom of the page in the September 21, 2022 post in Dr. Smith's ECG Blog ). Here are his publications.)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content