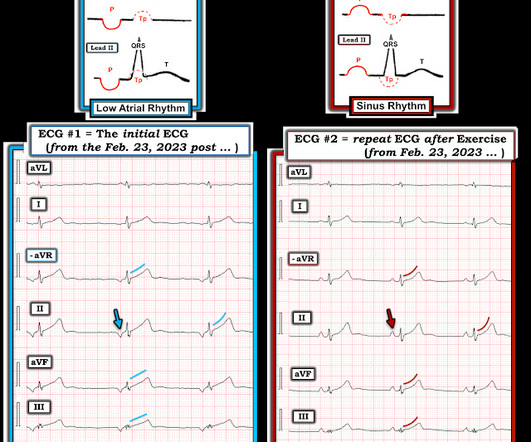
ECG Cases 48 – ECG Interpretation in Cardiac Arrest
Emergency Medicine Cases
FEBRUARY 13, 2024
The post ECG Cases 48 – ECG Interpretation in Cardiac Arrest appeared first on Emergency Medicine Cases.
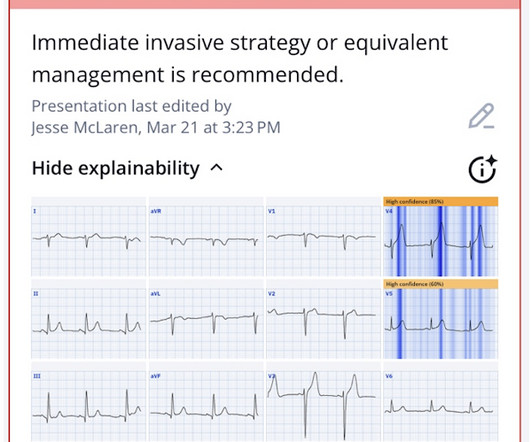
 Blog OR STEMI
Blog OR STEMI 
Emergency Medicine Cases
FEBRUARY 13, 2024
The post ECG Cases 48 – ECG Interpretation in Cardiac Arrest appeared first on Emergency Medicine Cases.

Emergency Medicine Cases
OCTOBER 22, 2019
In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. Can you identify which were early repolarization and which were anterior STEMI? The post ECG Cases 2: Early Repolarization or Anterior STEMI? appeared first on Emergency Medicine Cases.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
Emergency Medicine Cases
DECEMBER 16, 2019
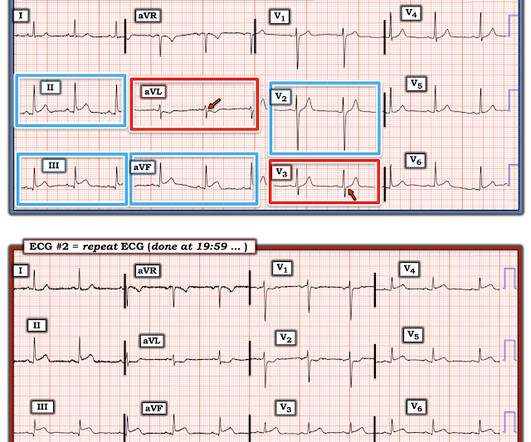
In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. The post ECG Cases 4: Lateral STEMI or Occlusion MI? Which had acute coronary occlusion? Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI.

Dr. Smith's ECG Blog
NOVEMBER 27, 2024
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria. Figure-1: ECG from the August 26, 2009 post in Dr. Smith's ECG Blog.
Emergency Medicine Cases
AUGUST 8, 2023
In this ECG Cases blog with Dr. Jesse McLaren we interpret 10 ECG cases and explore cardiac, metabolic and GI causes: We consider anginal equivalents, and look for ECG signs of Occlusion MI, including subacute occlusion from delayed presentations.
REBEL EM
SEPTEMBER 28, 2023
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. In these cases, thrombolysis is recommended to improve morbidity and mortality.
Dr. Smith's ECG Blog
OCTOBER 30, 2023
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).

Expert insights. Personalized for you.



























Let's personalize your content