This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. So, when I first began teaching ECGs and writing my books (in the early 1980s) — I decided to synthesize my impressions of the literature into what I felt (e.g. 2] Surawicz, B.
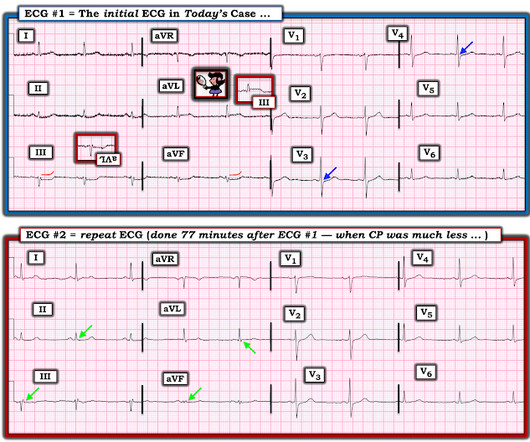
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? See these casese (and I have many others): First ED ECG is Wellens' (pain free). A 70-something y.o. male presents to triage with shortness of breath.
Turns out that it was a 50-something patient with no previous cardiac history who had called 911 for chest pain and had presented 75 minutes earlier by ambulance to triage (as the entire ED was overloaded). All triage ECGs are immediately shown to triage ED faculty.
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. The above principles are all well illustrated with this figure from my book, The ECG in Acute MI (2002). Computerized QTc = 419.
Note 2 other similar cases at the bottom that come from my book, The ECG in Acute MI. To the ED providers, the patient denied CP, SOB, or drug use. This is the ED bedside echo, recorded during ST elevation: Parasternal short axis shows huge concentric LVH. What do you think? Is there a formula to help with this?
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982 Apr;103(4 Pt 2):730-6. de Zwaan C et al. Am Ht J 117(3): 657-665; March 1989. Wehrens XH, Doevendans PA, Ophuis TJ, Wellens HJ.
Identifying patients with low risk for acute coronary syndrome without troponin testing: validation of the HEAR score. High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. It was obtained ~2 months prior to this patient's presentation in the ED. Am J Med 2021 5.
Her prehospital ECG was identical to her first ED ECG, and the cath lab was activated: There is massive ST elevation (greater than 15 mm) in V2 and V3, with ST elevation in I and aVL and reciprocal ST depression in II, III, aVF. This comes from chapter 28 of my book The ECG in Acute MI ). Peterson ED, Hathaway WR, Zabel KM, et al.
This is a re-posting of a Tweet by Robert Jones (@RJonesSonoEM), reproduced with permission, written by Pendell Meyers A middle aged female with history of smoking presented to the ED with "bad heartburn." Here is her prior baseline ECG (first), and her ED ECG (second): Baseline: ED ECG: What do you think?
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. LVH can mimic an acute anterior coronary occlusion (ACO) on the ECG. LVH usually has concave-upwards ST segments, but conVEX-upwards can also be seen, e.g. in these cases from Dr Smith’s book: The ECG in Acute MI : Case 22-1.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content