This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse Pines is the Chief Clinical Innovation at US Acute Care Solutions and a Clinical Professor and George Washington University and Professor of Emergency Medicine at Drexel University. In this role, he focuses on […] The post SGEM Xtra: I Wish that I Had Jesse’s Book first appeared on The Skeptics Guide to Emergency Medicine.
Background: The immediate post intubation period in the ED is a critical time for continued patient stabilization. The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. mg/kg over several minutes 0.02 – 0.1
A Multifaceted Intervention Improves Prescribing for Acute Respiratory Infection for Adults and Children in EmergencyDepartment and Urgent Care Settings. AEM July 2019 Guest Skeptic: Dr. Chris Bond is an emergency medicine physician and clinical lecturer in Calgary. It’s a great book to put on your reading list.
Case: You are working in the emergencydepartment (ED) and have just been involved in a difficult case in the resuscitation room. During the resuscitation, a relative of the patient you have been treating named Rudy makes a derogatory/rude comment about Emergency Medicine (EM) staff.
Battlefield acupuncture to treat low back pain in the emergencydepartment. Am J EM 2018 Guest Skeptics: Dr. Robert Edmonds is an emergency physician in the US Air Force in Virginia. Battlefield acupuncture to treat low back pain in the emergencydepartment. million visits per year in the US [1]. Al Sacchetti.
The emergencydepartment (ED) at UVA was rebuilt in 2019 and the department had not fully optimized its operations when COVID-19 hit. Following the pandemic, the ED saw a surge in its volume as it raced through 60,000 to 80,000 visits per year.
Child with Cough and Fever: Case Introduction A 6-year-old boy presents to the emergencydepartment complaining of cough for 3 days and fever for the last day. Distractions such as a toy, book, or phone/tablet can also help ease anxiety. ED Course The patient received antibiotics for pneumonia.
Clarke had begun an emergency medicine residency at what was then known as LA CountyUSC Hospital, Los Angeles. I was about two months into a family practice internship when I went to visit my uncle whose neighbor happened to be an ED resident, Dr. Clarke said. ED resident Dr. Steve Hui doing a pericardiocentesis on a trauma patient.
His health care focus included hospital efficiency, physician and patient satisfaction, and emergencydepartment (ED) wait times, as well as a host of nonhealth issues. Today, Dr. Morhaim is donating his time to a recently established Maryland commission focused on ED wait times. He got to be known as Dr. Dan.
ACEP President Speaks at Summit In October, ACEP President Dr. Aisha Terry spoke at the Summit on EmergencyDepartment Sickle Cell Care, and discussed point of care tools, standardization of care processes, improving ED care and more. Learn more at openbook.acep.org.
Lancet 2021 Case: You’re working a busy evening shift in your community emergencydepartment (ED) when a 58 year old female presents with a rapid onset terrible intensity headache. She has no significant headache history and you are concerned for subarachnoid hemorrhage so you order a head CT which confirms your suspicions.
Clinicians may under or over-estimate paediatric patients presenting to the ED as being at high-risk for sepsis if there do not have evidence-based heart and respiratory rate ranges, Brennan et al set out to add to our understanding of what is ‘normal ’ in paediatric vital signs. Acad Emerg Med. and one in the US by Bonafide et al.
Still, this wave of private equity acquisitions in emergency medicine has come crashing down on the heads of many early-career physicians. As of 2022, 1 in 4 emergencydepartments in the United States were staffed by a private equity-owned physician group. 2023 State of the Emergency Medicine Employer Market.
4 In an emergencydepartment (ED) presentation of cardiac arrest, the diagnosis of PE is challenging without the use of CT angiography. Point-of-Care-Ultrasound (POCUS) is a bedside modality that can assist Emergency Physicians (EPs) in differentiating PE from other causes of cardiac arrest. EKG RV strain. PMID: 24092475.
Emergency physicians have earned the right to “re-brand” ourselves as indispensable, money-saving change agents in the health care enterprise. Of course, the bill for any episode of emergencydepartment (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices.
ACEP also requires all exhibiting employers to have completed a profile in the ACEP Open Book encouraging greater transparency of group structure and policies. Topics include: Embracing Diversity in Medicine Working as a Female in the ED Brewing Success in the Transition from Resident to Attending What‘s Next? 28: 8 a.m.–5:30
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Here is the first ED ECG, with no pain: Sinus rhythm.
A prospective validation of the HEART score for chest pain patients at the emergencydepartment. External validation of the emergencydepartment assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP). Am J Emerg Med 2020 3. It was obtained ~2 months prior to this patient's presentation in the ED.
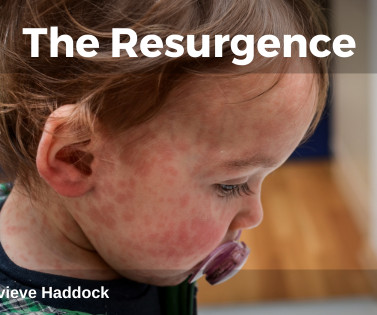
This leads to delay or misdiagnosis in the ED, which may lead to missed measles cases. Clear history taking In the EmergencyDepartment, healthcare professionals should prioritise thorough history-taking when assessing potential suspected cases. Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, Crowcroft NS.
The potential adverse patient effects of ambulance ramping, a relatively new problem at the interface between prehospital and ED care. Journal of Emergencies, Trauma and Shock, 1 (2) 129-129. Equitable Emergency Access: Rhetoric or reality? Emergency Medicine Australasia, 17 (4) 392-396. 2019/20 Annual Summary.
titled "The Association of Rocuronium Dosing and First-Attempt Intubation Success in Adult EmergencyDepartment Patients" revealed that first-attempt intubation success was the highest when more than 1.4 mg/kg of Succinylcholine during RSI in an ED setting." [1] mg/kg of Succinylcholine during RSI in an ED setting." [1]
Bupe Allergy Buprenorphine induction has been the mainstay of emergencydepartment treatment of opioid use disorder for more than a decade [11, 12]. Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). Some patients require re-dosing in the ED. 2023 [book]. Xylazine toxicity.
He is […] The post SGEM#337: Amazing GRACE-1 How Sweet the Guidelines – Recurrent, Low Risk Chest Pain in the EmergencyDepartment first appeared on The Skeptics Guide to Emergency Medicine. Date: July 1st, 2021 Guest Skeptic #1: Dr. Chris Carpenter is Professor of Emergency Medicine at Washington University in St.
Randomised control trial of adult therapeutic colouring for the management of significant anxiety in the EmergencyDepartment. AEM February 2020 Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Reference: Rajendran et al.
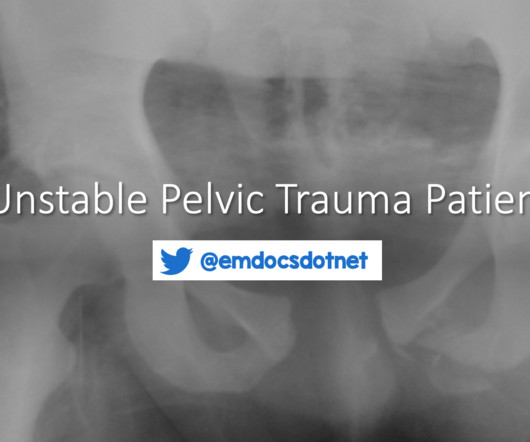
The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED. Figure 2: Open book pelvic fracture. This is less critical in ED management of the unstable pelvic fracture, as the optimal site for identification of rectal or vaginal tears is the operating room.
On the day of presentation, he woke up with a new rash over his face and hands which prompted the ED visit. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee on Infectious Diseases. Eczema herpeticum: making the diagnosis in the emergencydepartment. J Emerg Med.
Hypothermia Hypothermia, defined as core temperature less than 35oC (95oF) has been identified in up to 2/3 of trauma patients upon arrival to the emergencydepartment. Coagulopathy is identified through lab work in the emergencydepartment and is correlated in current literature with significantly worse patient outcomes.
Goldfrank’s Toxicologic Emergencies, 11e. Bombay: Kothari Book Depot; 1972. Mother states that the rash started as flat spots but then became raised bumps. J Infect Dis. 2021;224(12 Suppl 2):S379-S386. doi:10.1093/infdis/jiaa588 Suchard JR. Biological Weapons. In: Nelson LS, Howland M, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS.
The Pan American Health Organization also recommends screening anyone who was born in or lived longer than 6 months in a country with endemic Chagas as well as travelers with confirmed exposure to triatomines CD in the ED Most patients presenting with Chagas will be unaware of their infection status. EDs in the U.S. de Oliveira, E.C.
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 She is sent to the medical ward after three days in the ED with the diagnoses of resolving septic shock, severe malaria, and AKI.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content