This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this role, he focuses on […] The post SGEM Xtra: I Wish that I Had Jesse’s Book first appeared on The Skeptics Guide to Emergency Medicine. This is the book that can help clinicians achieve that goal. This fantastic book provides answers to those questions in a brief and helpful way.
Read the series Buy the print book! In: Fleisher and Ludwig’s Textbook of Pediatric Emergency Medicine, 7th ed, Shaw K, Bachur RG (Eds), Lippincott Williams & Wilkins, Philadelphia 2015. All revolve around understanding zipper anatomy and obtaining adequate exposure to assess how the skin is entrapped.
Background: The immediate post intubation period in the ED is a critical time for continued patient stabilization. The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. Short acting. mg/kg IV followed by 0.05 – 0.4
Getting into flow is often linked with being engaged in life or death activities, something that we as ED physicians are intimately failure with on a regular basis. Does the high stakes life or death environment in the ED allow us to access a flow state, even though our own lives are not at risk? But what about the rest of us?
At one of the hospitals, while my partner finished up the run form in the passenger seat –shed teched the call–I announced I was going back into the ED to the EMS room to see if they had any pizza. The young man told her then I had written some books about being a paramedic that she should read. Eat pizza or read a book.
Case: You are working in the emergency department (ED) and have just been involved in a difficult case in the resuscitation room. A better option is to try kindness as outlined in the excellent book by Dr. Brian Goldman. We discussed Brian’s book on the SGEM Xtra called Don’t Give Up – The Power of Kindness.
I was about two months into a family practice internship when I went to visit my uncle whose neighbor happened to be an ED resident, Dr. Clarke said. ED attendings Dr. Gerald Whelan and Dr. Shumary Chow supervising a full arrest in C booththe main trauma roomwith an ED tech administering CPR. Click to enlarge.)
Distractions such as a toy, book, or phone/tablet can also help ease anxiety. When there is lung pathology, the consolidation or fluid allows for direct visualization of the pathology with lung POCUS and replaces the air artifacts. The patient should be in a position of comfort: supine, sitting, or in parent’s lap (Figure 1).
Aisha Terry spoke at the Summit on Emergency Department Sickle Cell Care, and discussed point of care tools, standardization of care processes, improving ED care and more. Vetted details, unparalleled access, and actionable insights about group structure, leadership, policies and more, make ACEP Open Book an indispensable resource.
His health care focus included hospital efficiency, physician and patient satisfaction, and emergency department (ED) wait times, as well as a host of nonhealth issues. Today, Dr. Morhaim is donating his time to a recently established Maryland commission focused on ED wait times. His path toward state legislative work was set.
Lancet 2021 Case: You’re working a busy evening shift in your community emergency department (ED) when a 58 year old female presents with a rapid onset terrible intensity headache. Date: March 11th, 2021 Guest Skeptic: Dr. Robert Edmonds is an emergency physician in the US Air Force in Ohio. Reference: Post et al. Reference: Post et al.
Background: Lower back pain is one of the most common emergency department (ED) complaints, comprising approximately 2.6 Opioids are frequently used in the ED to treat pain and ED physicians are among the most frequent prescribers of opioids [2]. million visits per year in the US [1].
So, when I first began teaching ECGs and writing my books (in the early 1980s) — I decided to synthesize my impressions of the literature into what I felt (e.g. Upon arrival he was found alert and oriented, and without gross distress. He denied difficulty breathing, epigastric pain, or chest discomfort. Figure 1-2. Is it LBBB, or LAFB?
On today’s show, Ed interviews the host of The Medic Mindset podcast, Ginger Locke. We also talk about a few books that might change your practice, or how you think. We also talk about a few books that might change your practice, or how you think. How do you learn? How do your students learn? How do you learn?
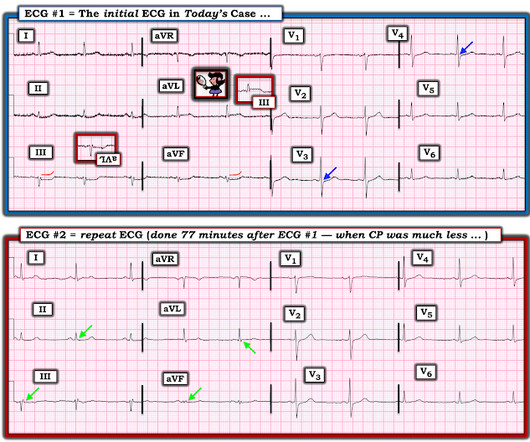
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? See these casese (and I have many others): First ED ECG is Wellens' (pain free). A 70-something y.o. male presents to triage with shortness of breath.
Clinicians may under or over-estimate paediatric patients presenting to the ED as being at high-risk for sepsis if there do not have evidence-based heart and respiratory rate ranges, Brennan et al set out to add to our understanding of what is ‘normal ’ in paediatric vital signs. What did previous studies show? What is the problem?
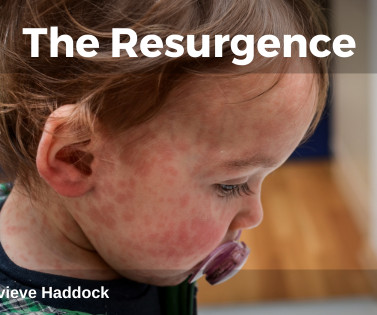
This leads to delay or misdiagnosis in the ED, which may lead to missed measles cases. The reduced coverage is particularly notable in urban areas like London , where socio-economic and cultural barriers further compound the problem. This contributed to a sharp increase in cases of both diseases in 2024.
4 In an emergency department (ED) presentation of cardiac arrest, the diagnosis of PE is challenging without the use of CT angiography. Case A 25-year-old-female presented to the ED in cardiac arrest. 1-3 As many as 25% of acute PE cases present as sudden cardiac death.
Note 2 other similar cases at the bottom that come from my book, The ECG in Acute MI. To the ED providers, the patient denied CP, SOB, or drug use. This is the ED bedside echo, recorded during ST elevation: Parasternal short axis shows huge concentric LVH. What do you think? See discussion at the bottom.
Turns out that it was a 50-something patient with no previous cardiac history who had called 911 for chest pain and had presented 75 minutes earlier by ambulance to triage (as the entire ED was overloaded). All triage ECGs are immediately shown to triage ED faculty. The lesion was of course Stented. In this context.
From 200 billion dollars that year, the firms that make up the Healthcare Private Equity Association now have over 2 trillion dollars in assets under management. 5 Private equity follows a fundamentally different business model from other forms of investment, such as publicly-traded or privately-owned companies.
I’ve read all his books, seen him live, and watched all of his series. In his book, Kitchen Confidential , he talks about the business of cooking food a lot like colleagues I know talk about EMS. In one of the better parts of this book, he shares with you a typical day of his from waking up to end. Kind of like EMS.
The emergency department (ED) at UVA was rebuilt in 2019 and the department had not fully optimized its operations when COVID-19 hit. Following the pandemic, the ED saw a surge in its volume as it raced through 60,000 to 80,000 visits per year. The ED went from daily volumes of 180 patients per day [PPD] to over 210 PPD.)
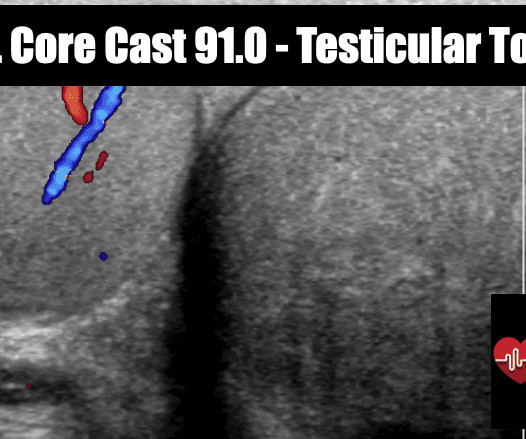
Clinical predictors for testicular torsion as seen in the pediatric ED. Epidemiology: Most common cause of acute scrotal pain in prepubertal boys Torsion present in 3.2% Epidemiology: Most common cause of acute scrotal pain in prepubertal boys Torsion present in 3.2% OR = 58.8 (Ben-Israel 10, (-) LR = 0.13 Am J Emerg Med 2010; 28:786-789.
I apologize in advance to Sebastian Junger and his excellent book, The Perfect Storm. If you’ve read it or seen the movie with Mark Wahlberg; (and you should read the book), you know it’s about a combination of circumstances that come together in an unprecedented way to cause devastation. What do you notice? And then, reality sets in.
When I arrived in the ED, I sought out the team leader to receive my assignment. Books, blogs, and mentors have suggested that women should try to emulate traditionally “masculine” characteristics when leading (e.g. A gruff nudge jerked me awake from a brief two hours of sleep. Team members were taking their positions.
Of course, the bill for any episode of emergency department (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices. Now, many acute pyelonephritis patients receive an IV antibiotic, analgesia, and an antiemetic in the ED.
ACEP also requires all exhibiting employers to have completed a profile in the ACEP Open Book encouraging greater transparency of group structure and policies. Topics include: Embracing Diversity in Medicine Working as a Female in the ED Brewing Success in the Transition from Resident to Attending What‘s Next?
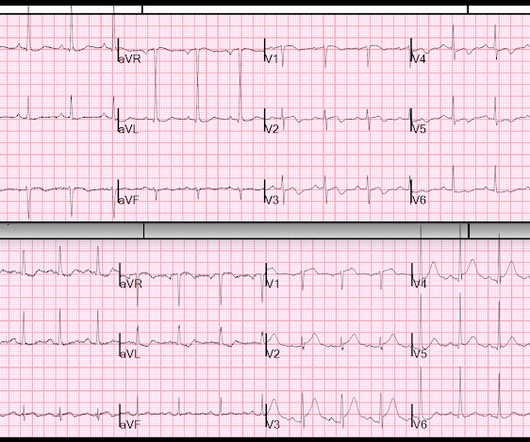
Her prehospital ECG was identical to her first ED ECG, and the cath lab was activated: There is massive ST elevation (greater than 15 mm) in V2 and V3, with ST elevation in I and aVL and reciprocal ST depression in II, III, aVF. This comes from chapter 28 of my book The ECG in Acute MI ). hours when she called 911.
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. The above principles are all well illustrated with this figure from my book, The ECG in Acute MI (2002). Computerized QTc = 419.
The potential adverse patient effects of ambulance ramping, a relatively new problem at the interface between prehospital and ED care. We teach them to use this education in recognising disease states for urgent intervention on scene, and timely transport aimed at improving patient outcomes. DOI: 10.4103/0974-2700.43201 Kennedy, M.
WHAT brought this 1st patient to the ED on the day he presented — which was no less than 3 weeks after the onset of his symptoms? C ASE # 2: The history in the 2nd Case was " 3 weeks of exertional chest pain" — in this patient who was "painfree on arrival" in the ED. Specifying the level is more accurate, evidence-based and safe 3.
"What is the difference between assist control and SIMV?" This is a question I would get all the time, or at least some variation of it. A while back, a colleague asked me this question to answer on the RSI podcast. For anyone who uses the Hamilton and is reading this may be asking, "Did you say A/C and SIMV modes?"
This is a re-posting of a Tweet by Robert Jones (@RJonesSonoEM), reproduced with permission, written by Pendell Meyers A middle aged female with history of smoking presented to the ED with "bad heartburn." Here is her prior baseline ECG (first), and her ED ECG (second): Baseline: ED ECG: What do you think?
I had a reputation as a tough preceptor. I was the one that people either sought out because they wanted the challenge; or the one that they avoided. No immortal number to place you on the long line of paramedics, going back to license number 1. It may or may not be true. But the connotation, especially as a student, was there. That was it.
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
I believe that I was the first to represent Wellens as a reperfusion syndrome, in my book , The ECG in Acute MI , pages 22-23 and 51, and in chapter 27 on Reperfusion and Reocclusion. From my experience, I am confident that if it were formally studied, it would be born out. Wehrens XH, Doevendans PA, Ophuis TJ, Wellens HJ. Am Heart J.
I also find the following information useful: Succinylcholine has an onset of approximately 45 seconds, whereas Rocuronium has an approximate onset of 60 to 90 seconds -- Depending on what book you read. mg/kg of Succinylcholine during RSI in an ED setting." [1] mg/kg of Succinylcholine during RSI in an ED setting." [1]
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. LVH usually has concave-upwards ST segments, but conVEX-upwards can also be seen, e.g. in these cases from Dr Smith’s book: The ECG in Acute MI : Case 22-1. Is the ST elevation due to LVH? 3 Is the STE concave or convex?
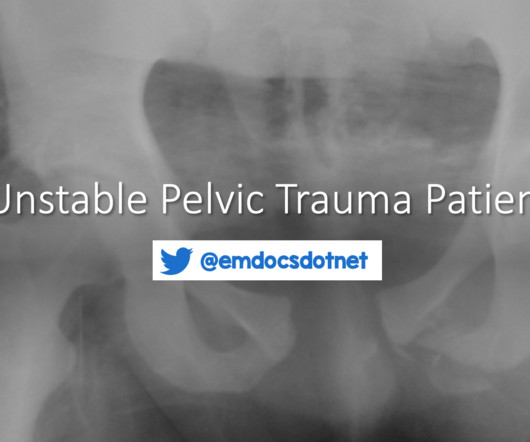
The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED. Her initial vital signs are blood pressure 76/54 mmHg, heart rate 128 bpm, temperature 37.0˚ C, respiratory rate 20 breaths per minute, and oxygen saturation 95% on room air. of pelvic fractures to be open.
Case: One night during an overnight shift, you are taking care of a patient who presented to the emergency department (ED) due to anxiety and vague suicidal ideation. Background: Psychological disorders are a common reason for presenting to the ED. The ED itself can be a stressful environment and exacerbate anxiety.
Recently, a pediatric patient presented to the ED who just returned from abroad with a gastroenteritis presentation. The CDC Yellow Book app 2018. Post-COVID everyone seems to be posting the perfect picture of their travels to the far reaches of the world. In addition to my passion for PEM, I also share a passion for global health.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content