This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
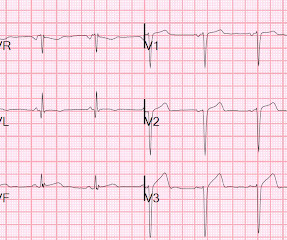
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Is it normal STE? This is a "Transient OMI".
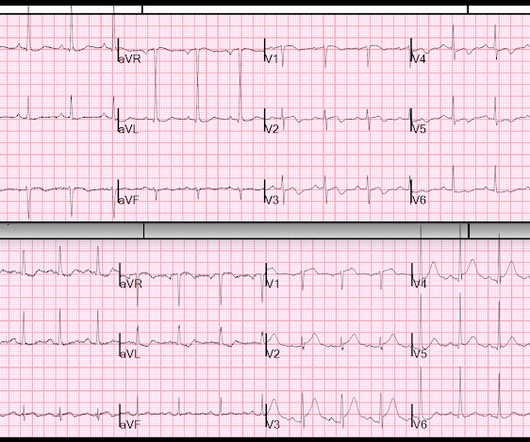
Note 2 other similar cases at the bottom that come from my book, The ECG in Acute MI. This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. To the ED providers, the patient denied CP, SOB, or drug use. What do you think?
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic."
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. The above principles are all well illustrated with this figure from my book, The ECG in Acute MI (2002). Computerized QTc = 419.
Her prehospital ECG was identical to her first ED ECG, and the cath lab was activated: There is massive ST elevation (greater than 15 mm) in V2 and V3, with ST elevation in I and aVL and reciprocal ST depression in II, III, aVF. This comes from chapter 28 of my book The ECG in Acute MI ). Peterson ED, Hathaway WR, Zabel KM, et al.
Of course, the bill for any episode of emergency department (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices. Now, many acute pyelonephritis patients receive an IV antibiotic, analgesia, and an antiemetic in the ED. This process required at least a full day.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Specifying the level is more accurate, evidence-based and safe 3.
See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? It even meets STEMI criteria: 2.5 I believe that I was the first to represent Wellens as a reperfusion syndrome, in my book , The ECG in Acute MI , pages 22-23 and 51, and in chapter 27 on Reperfusion and Reocclusion.
This is a re-posting of a Tweet by Robert Jones (@RJonesSonoEM), reproduced with permission, written by Pendell Meyers A middle aged female with history of smoking presented to the ED with "bad heartburn." Here is her prior baseline ECG (first), and her ED ECG (second): Baseline: ED ECG: What do you think?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content