This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
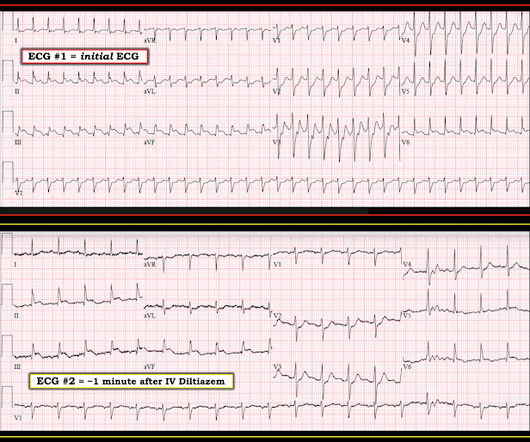
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. This was deemed “non-specific” by the ED physicians. Type I ischemia.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. Each main coronary artery (LAD, RCA and LCx) are shown in separate images. There are no coronary stenoses.
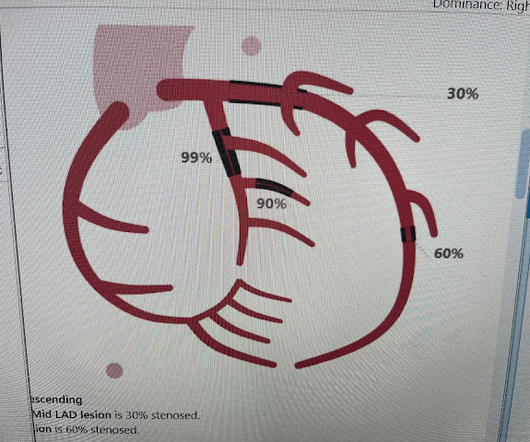
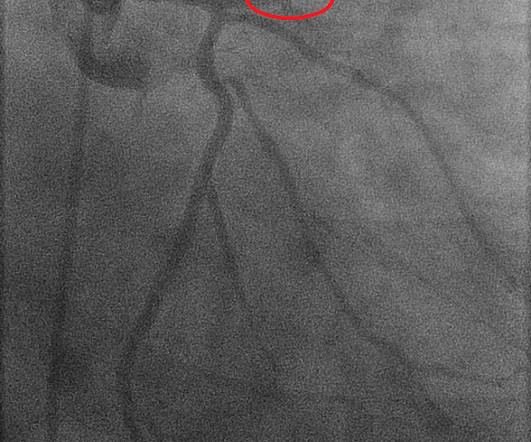
Angiogram: Severe two-vessel coronary artery disease with possible co-culprits (90% proximal circumflex, 70% mid/distal RCA) in the setting of non-ST elevation myocardial infarction. Marked ST depression from multi-vessel coronary disease serves to attentuate what would have been ST elevation in leads II and aVF ).
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD CAD-RADS category 1. --No Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
Angiography showed normal coronaries. A followup ECG was recorded 2 days later: No definite evidence of infarction. MINOCA: Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease). Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus."
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. It can only be seen by IVUS.
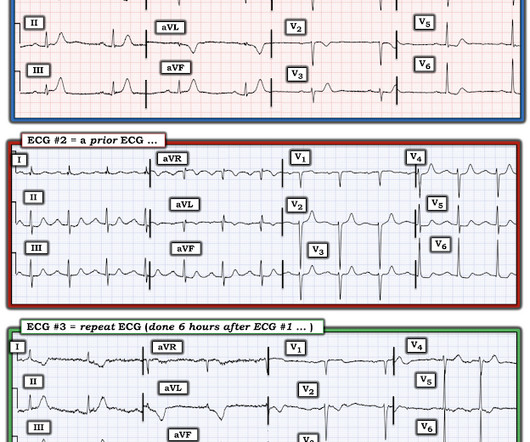
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted. What Do We Learn from ECG #3 ?
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Lead aVL, for example, has a definite J-wave. Stat echo would also be helpful. Teaching points: 1.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Second , the increased demand created by extreme tachycardia may exceed the ability of the coronary arteries to supply sufficient blood (due to preexisting three vessel or left main disease, with or without ACS). But this is not definite because the angiogram was not done at the same time as the ECG changes suggesting OMI.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. The QRS duration is 118 ms , so by definition it is not Left Bundle Branch Block (which must be 120 ms at a minimum and is usually longer) Thus, LVH on the ECG does not always correlate with anatomic LVH. What do you think? There is LVH.
He also had non-acute CAD of the RCA (50%) and LCX (50%). This is a h igher - p revalence H istory for acute coronary disease. B OTTOM L ine : While ECG #1 does not satisfy the definition of a STEMI — as per Dr. Meyers, it really looks like a cute L AD O MI. Cath images: Before intervention.
Lead I has a definitively hyperacute T-wave without STE. She also had non-acute CAD of the left main (50%) and LCX (75%). Compared with sustained STEMI, transient STEMI was associated with less myocardial damage, less extensive coronary artery disease, higher TIMI flow grade, and better cardiac function. They opened it.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. Use STEMI criteria to identify acute coronary occlusion: the ECG was STEMI negative 2. Below is the ECG. What do you think?
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
No prior similar symptoms or known CAD. Here is the repeat 12 Lead ECG approximately 20 minutes later (still pain free) Now it shows definite reperfusion More inferior T-wave inversion Less STD in V2, V3. post OMI with significant multi-vessel coronary disease. He took two full strength aspirin prior to EMS arrival.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out." But that is not what happened.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He looked back in time in the patient's chart and saw these ECGs and immediately recognized that they manifested subtle OMI. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content