This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronary artery disease. 2. Coronary angiography reveals significant and severe CAD involving all three epicardial vessels. He awoke earlier that morning in his usual state of health. Type I ischemia.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? He has no history of coronary artery disease. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. AEM June 2022.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. This patient in today's case was a man in his 60s with a known history of coronary disease, including prior stents. This is a re-post of an excellent case from 2021.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. Each main coronary artery (LAD, RCA and LCx) are shown in separate images. There are no coronary stenoses.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT.
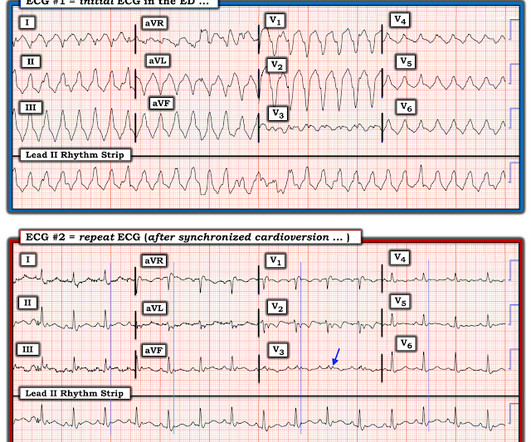
Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis. There was no obvious pallor, diaphoresis, or dyspnea, and he denied any prior episodes of vomiting. But the lesion is still active!
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. A 12 Lead ECG was recorded. It’s important to stress the presence of a normal QRS (i.e., 2] Driver, B.
The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Initial hsTnI was 384 ng/L. The report describes a 60% proximal LAD lesion with TIMI 3 flow.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. Cardiology admitted him for observation with plans for next-day coronary angiogram. A 56 y/o Male called 911 from his hotel room in the early morning hours after abruptly awakening from sleep with crushing chest discomfort and difficulty breathing.
Angiogram: Severe two-vessel coronary artery disease with possible co-culprits (90% proximal circumflex, 70% mid/distal RCA) in the setting of non-ST elevation myocardial infarction. Marked ST depression from multi-vessel coronary disease serves to attentuate what would have been ST elevation in leads II and aVF ).
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAFB) on the admission ECG.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD CAD-RADS category 1. --No Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45
He has a history of known CAD, diabetes, and dyslipidemia. The ED ECG in the context of the prehospital ECGs was indeed diagnostic of acute coronary occlusion. Cath Results: The cath lab was activated and co-culprit lesions were found: 99% circumflex and 95% right coronary artery (RCA). Both were stented.
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
Angiography showed normal coronaries. MINOCA: Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease). Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." 2) overlooked obstructive coronary disease (e.g., The K was normal.
In this category, most cases are a result of end-stage coronary artery disease, either with a history of myocardial infarction or with a chronically underperfused, yet viable, myocardium. This may be further subdivided into systolic or diastolic heart failure. In many patients, both processes are present simultaneously. Currently, 5.7
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chest pain or shortness of breath. PM Cardio digitized version.
Pervasive use of CT coronary angiography has been an unnecessary feature of the evaluation of patient with low-risk chest pain for the better part of a decade now. Patients were eligible by symptoms of an acute coronary syndrome, supported by ECG changes, an elevated troponin, or a history of ischemic heart disease.
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. Increased risk in those with preexisting CKD, other risk factors for renal disease (HTN or CAD), and those on ACEIs/ARBs.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. No similar symptoms in the past. He denied headache or neck pain associated with exertion. No further troponins were measured.
She had zero CAD risk factors. Next day, t he patient was taken for an angiogram and found to have a reperfused LAD lesion with good flow that appeared to the angiographer as if it was a spontaneous coronary artery dissection. hours of substernal chest pressure. Here was her ECG at time zero: What do you think? The lesion was stented.
This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries. 1 Despite the rarity of dextrocardia, coronary artery disease can occur with a similar frequency to that of the general population. Coronary heart disease in situs inversus totalis.
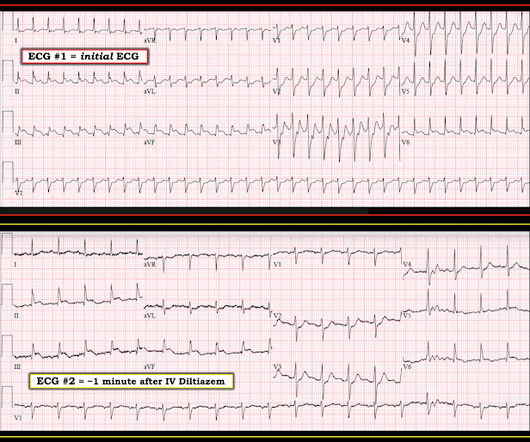
He had a history of CAD with CABG. Ventricular fibrillation is not only caused by acute coronary syndrome. A middle-aged male had a V Fib arrest. He had not complained of any premonitory symptoms (which is very common). Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. He did not have ACS.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. V1 has 0.5 mm of elevation.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
As the pregnant population continues to age and with RF and smoking and DM still common we can expect to see pregnant woman with CAD. Some unique features to consider in pregnancy is spontaneous coronary artery dissections. Improved care of complex. Read More » Welcome back to the tasty morsels of critical care podcast.
The ED provider ordered a coronary CT scan to assess the patient for CAD. The patient was taken emergently to the cath lab for a pericardiocentesis instead of a coronary angiogram. Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. It is not a missed STEMI, but it is a missed coronary occlusion. Wang T, Zhang M, Fu Y, et al.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Instantaneous wave-free ratio is performed using high fidelity pressure wires that are passed distal to the coronary stenosis. We need to do some more investigation.
He had a family history of early CAD and occasional drug and tobacco use. However, subtle coronary occlusion may be completely missed by the computer and called "normal." An ECG is recorded and the computer reads it as "normal". Do you want to see it? Or would you rather not be bothered? I'd rather be bothered. References : 1.
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. There is clearly a wide complex tachcyardia (although the QRS duration is not far above 120msec). Or it could simply still be classic VT. RVEF 100 ml/m2.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
A middle-aged male with h/o CAD and stents presented with typical chest pressure. Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAFB) on the admission ECG.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). There is also STD in V2-V4 (but maximal in V5-V6).
Is this due to coronary occlusion? The medic activated the cath lab but was refused by the interventionalist, who did not believe that this ECG represented acute coronary occlusion. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion.
Second , the increased demand created by extreme tachycardia may exceed the ability of the coronary arteries to supply sufficient blood (due to preexisting three vessel or left main disease, with or without ACS). Therefore this patient is either in some form of SVT or atrial flutter. Fatigued-appearing but mentating perfectly. Clear lungs.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. Several hours prior to presentation, while driving his truck, he started experiencing new central chest pain, without radiation, aggravating/alleviating factors, or other associated symptoms. No acute culprit. He was admitted to cardiology. Pericarditis?
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. LVH can mimic an acute anterior coronary occlusion (ACO) on the ECG. There is ST elevation, but also high voltage (though the high voltage is NOT in the leads with worrisome STE, rather, it is in aVL).
The patient was transferred immediately for angiogram which revealed no significant CAD, and no intervention was performed. Coronary spasm causing massive current of injury with shark fin ECG. I would not expect ST-E to vanish in four beats with dissolving thrombus (also we know that the coronaries were clean).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content