This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
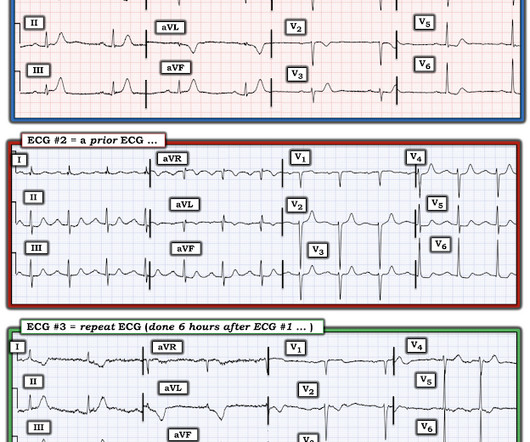
Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis. it has been subsequently deemed a STEMI-equivalent. But the lesion is still active!
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. His vital signs were unremarkable, and the lung fields were free of fluid congestion during auscultation.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. We've come a long way in 2 years!
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery? Widimsky P et al.
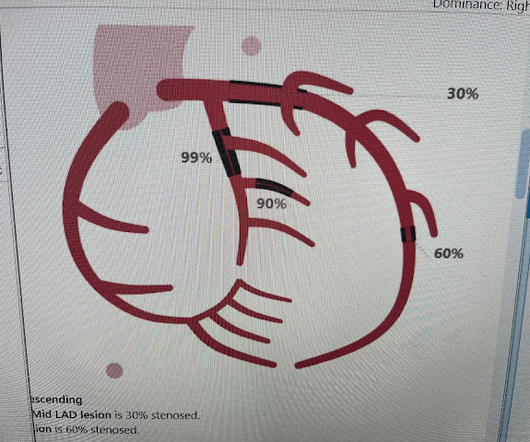
20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. Angiogram: Severe two-vessel coronary artery disease with possible co-culprits (90% proximal circumflex, 70% mid/distal RCA) in the setting of non-ST elevation myocardial infarction.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD CAD-RADS category 1. --No Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45
He has a history of known CAD, diabetes, and dyslipidemia. The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. The ED ECG in the context of the prehospital ECGs was indeed diagnostic of acute coronary occlusion.
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries. Figure 1: EKG for Dextrocardia showing STEMI. The second EKG was concerning for STEMI in the precordial leads (see figure 1). Click to enlarge.) 1 It has a prevalence of 0.01
Angiography showed normal coronaries. This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. Troponin I rose to 44.1
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. His ECG was repeated at this point: This shows a well developed anterior STEMI. The peak troponin I was over 100.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e STEMI , ST-segment elevation acute myocardial infarction ). I B Ambulance personnel must be trained and equipped to identify STEMI and administer fibrinolysis if necessary.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic."
He had a history of CAD with CABG. Ventricular fibrillation is not only caused by acute coronary syndrome. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. A middle-aged male had a V Fib arrest. He had not complained of any premonitory symptoms (which is very common). Learning Points: 1.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. It can only be seen by IVUS.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Most recent echo showed EF of 60%. Learning Points: 1.
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. This was my response: "This looks like a worrisome EKG. But by now you must have a repeat ECG.
The ED provider ordered a coronary CT scan to assess the patient for CAD. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!)
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. Pericarditis?
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He had a family history of early CAD and occasional drug and tobacco use. He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality.
She had zero CAD risk factors. It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. The lesion was stented.
As the pregnant population continues to age and with RF and smoking and DM still common we can expect to see pregnant woman with CAD. Some unique features to consider in pregnancy is spontaneous coronary artery dissections. Valve disease provides the most interesting part of obstetric care.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Is this due to coronary occlusion? The medic activated the cath lab but was refused by the interventionalist, who did not believe that this ECG represented acute coronary occlusion. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Look at the aortic outflow tract.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? In this case, there is diffuse ischemic ST depression of subendocardial ischemia, of course with accompanying reciprocal STE in aVR.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. The medics were worried about STEMI, as it meets STEMI criteria. Discussion Thus, no further ECGs were recorded and there was no angiogram or stress test or CT coronary angiogram. There was no prodrome and no associated symptoms such as SOB or CP.
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? He also had non-acute CAD of the RCA (50%) and LCX (50%).
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). He had multiple cardiac arrests with ROSC regained each time.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? A repeat ECG was performed and cardiology was re-consulted: Roughly unchanged. No acute culprit. Pericarditis?
In this study of dialysis patients with severe CAD, 77% had an abnormal resting EKG and the most common abnormality was LVH. Another reason may be that the EKG is more difficult to interpret in patients with dialysis due to baseline abnormalities, including LVH. Herzog et al.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Below is the ECG. Take home 1.
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
No prior similar symptoms or known CAD. The Queen of Hearts Diagnosed "STEMI/STEMI equivalent" on that first ECG (she now uses "STEMI Equivalent" rather than OMI). The fact that she states "STEMI-Equivalent" here means that she does not think it is reperfused, but she does not know that the patient is pain free now.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out." But that is not what happened.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content