This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
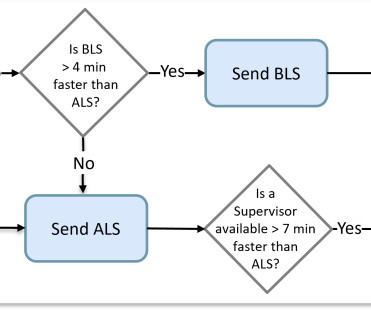
Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance. It was a matter of determining which crew was available closest to the scene. Life-threatening requests are similarly streamlined.
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. He awoke earlier that morning in his usual state of health.
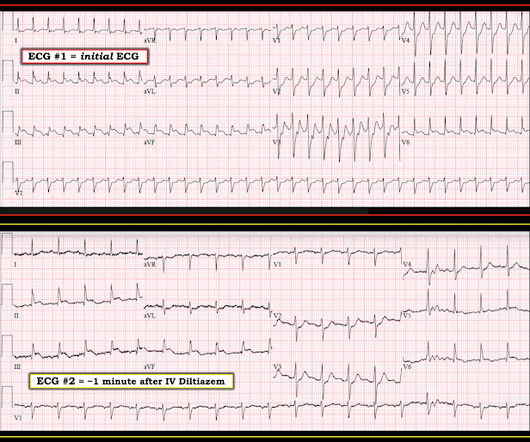
Hosts: Brian Gilberti, MD Jonathan Kobles, MD [link] Download Leave a Comment Tags: Cardiology Show Notes Understanding AF with RVR Categories General AF with RVR: Definition and basic understanding. Metoprolol Considerations: Dosing (5 mg every 10-15 minutes, max 15 mg), benefits in CAD and HF, limitations in asthma/COPD patients.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. How would you assess this ECG? How confident are you in your assessment? What is your next step? How did the Queen do?
My thought process in the moment was that leads aVL and V2 display an ST-segment that is “inappropriately baseline” – not elevated, by definition, but may very well be an equivalent of such as the ischemic zone is actively “pushing” them in an upward manner. This results in Type I MI. This results in Type II MI. Does the ECG normalize?
She had a normal EF, and no significant CAD, and was taking flecainide to suppress the AF. So, while the “ Bottom LINE ” is that we do not have a definitive answer — in the interest of academic discussion, I’ll present my rationale for why I believe the initial ECG shows AFlutter ( and not VT ) , in this patient with Flecainide toxicity.
Patient stated that he has had glucose over 400 even though he has not missed any doses of insulin. Aslanger's is a combination of inferior OMI with widespread ST depression and is due to BOTH occlusion of one artery (usually the circumflex, but sometimes the RCA) AND simultantous 3 vessel disease.
He had no previous history of CAD, and presented with very typical waxing and waning chest pain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. This is all suggestive of posterior STEMI, but not definitely diagnostic. I saw this 59 year old male 3 weeks ago.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chest pain or shortness of breath. PM Cardio digitized version.
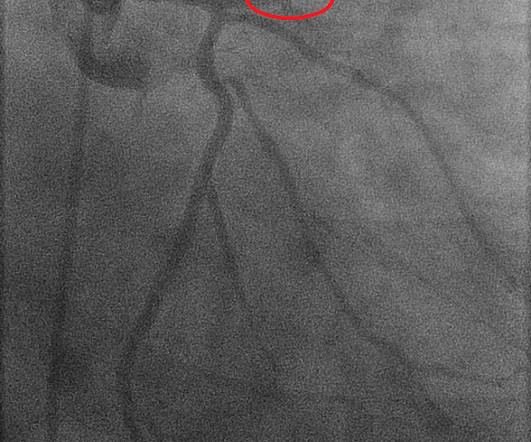
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. Angiography Angiography was performed after aspirin and heparin were started.
A followup ECG was recorded 2 days later: No definite evidence of infarction. Diagnosis of MINOCA should be made according to the Fourth Universal Definition of MI, in the absence of obstructive coronary artery disease (CAD) (no lesion ≥50%). She then had a 12-lead: What do you think? There is sinus bradycardia with one PVC.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. He was diagnosed as NSTEMI.
CAD-RADS category 1. --No The most remarkable finding on ECG #1 — is fairly shallow but-definitely-present T wave inversion in leads V1-thru-V5. A repeat troponin returned at 0.45 ng/mL, consistent with reperfused OMI, or Non-OMI. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island. I remember Allie well from her days in the Research volunteer program at Hennepin. F (rectal). There was a 0.9%
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. V1 has 0.5 mm of elevation. ng/mL [IQR: 0.46, 2.35].
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Lead aVL, for example, has a definite J-wave. Stat echo would also be helpful.
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
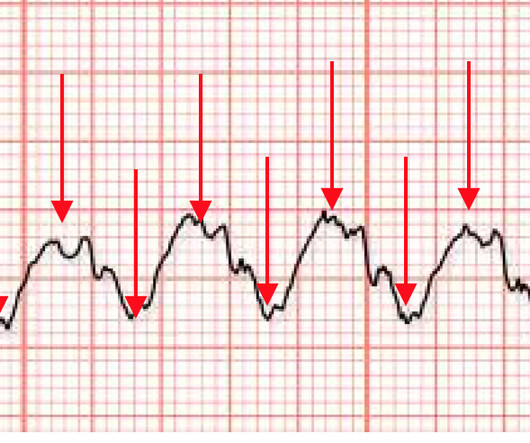
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrial flutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrial flutter. Fatigued-appearing but mentating perfectly.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. The QRS duration is 118 ms , so by definition it is not Left Bundle Branch Block (which must be 120 ms at a minimum and is usually longer) Thus, LVH on the ECG does not always correlate with anatomic LVH. What do you think? There is LVH.
Lead I has a definitively hyperacute T-wave without STE. She also had non-acute CAD of the left main (50%) and LCX (75%). This ECG shows persistent Occlusion MI but does not meet STEMI criteria. V2 still has STE and hyperacute T-waves. There is a new Q-wave in aVL, with STE and large T-wave as well. II, III, aVF, and V6 have STD.
We found the address matching that of a farm, but the message on our CAD (Computer Assisted Dispatch System) said the location was towards the back of the farm and in a trailer. Sure doesn’t match the description we were given by dispatch, definitely not a ladies house! Me: “Pretty quiet here.”
He also had non-acute CAD of the RCA (50%) and LCX (50%). B OTTOM L ine : While ECG #1 does not satisfy the definition of a STEMI — as per Dr. Meyers, it really looks like a cute L AD O MI. Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes.
As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. Below is the ECG. What do you think? There’s sinus bradycardia, first degree AV block, normal axis, delayed R wave progression, and normal voltages.
No prior similar symptoms or known CAD. Here is the repeat 12 Lead ECG approximately 20 minutes later (still pain free) Now it shows definite reperfusion More inferior T-wave inversion Less STD in V2, V3. He arrived at the ED just shy of two hours after onset, pain free. PMHX significant for hypertension and BPH.
The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. Pre-intervention. In other words, millimeters really don't matter!
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out."
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He looked back in time in the patient's chart and saw these ECGs and immediately recognized that they manifested subtle OMI. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content