This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System.
NERIS’s ultimate goal is to save lives through the power of data , which means it will continue to evolve and improve over time to ensure the industry has what it needs to document and keep up with new and evolving threats. With API , participating CAD and RMS vendors will be able to automatically send data back and forth to NERIS.
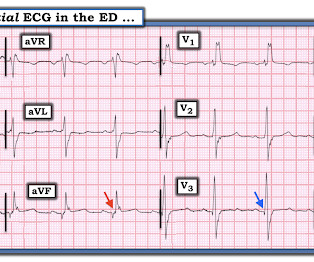
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. So I made an ED diagnosis of Non-Occlusion Myocardial Infarction (NOMI), and his next day angiogram confirmed NOMI. Figure-1: The initial ECG that was done in the ED ( See text ). Here is his initial ECG: What do you think?
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergency department (ED). This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. There is no further workup at this time.
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documentedCAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Here is his ED ECG: There is obvious infero-posterior STEMI. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia."
The note documents that the first view of the LCX showed 99%, TIMI 2 flow, but then (before intervention) was seen to fully occlude in real time (100%, TIMI 0). The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Pre-intervention.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He was worked up non-emergently in the ED with pain recurring and resolving multiple times during his stay. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content