This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
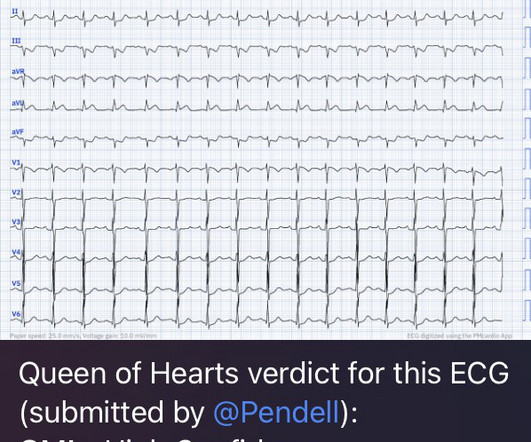
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Diagnosis of Type I vs. Type II Myocardial Infarction in EmergencyDepartment patients with Ischemic Symptoms (abstract 102).
Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Background: Chest pain is one of the most common presentations to the ED.
Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. The ST changes went overlooked by both the ED physician and the on-call cardiologist, and the patient was subsequently admitted to telemetry. A 12 Lead ECG was recorded: This is pathognomonic for classic deWinter T waves, indicative of LAD occlusion.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. I could have told you this (and did tell you this) without an MRI.
She was unable to be defibrillated but was cannulated and placed on ECMO in our EmergencyDepartment (ECLS - extracorporeal life support). Diagnosis of MINOCA should be made according to the Fourth Universal Definition of MI, in the absence of obstructive coronary artery disease (CAD) (no lesion ≥50%). myocarditis).
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergencydepartment (ED). The patient initially presented to an outside ED and was subsequently transferred to our facility for continuity of care.
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol. No more troponins were obtained.
This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. Usefulness of automated serial 12-lead ECG monitoring during the initial emergencydepartment evaluation of patients with chest pain. Ann Emerg Med 1998;31(1):3-11. See image below: Slow upstroke, fast downstroke.
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent case 1 below of a 100% LM occlusion. Beware crescendo angina in patient with known CAD ST Elevation in aVR Case 7.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the EmergencyDepartment for acute chest pain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. Scattered other nonobstructive CAD.
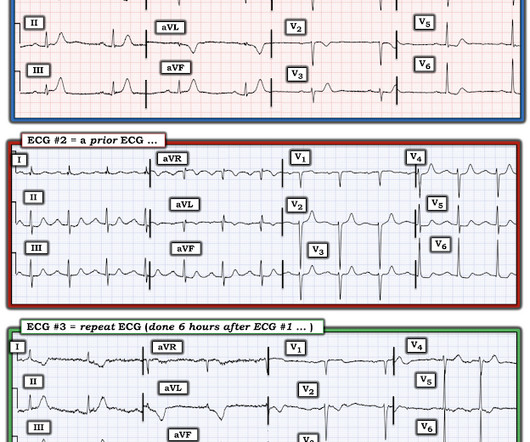
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. The Repeat ECG: As per Dr. McLaren — the patient was unfortunately discharged from the ED — but returned 6 hours later with a recurrence of chest pain.
These are very commonly encountered in the emergencydepartment, so being able to correctly identify the rhythm is extremely important. He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. This week, we are finishing 4 of a 4-part series tackling tachydysrhythmias. Lets dive in! Take a look: Figure 3.
She presented to the EmergencyDepartment at around 3.5 The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Patients with complete left main occlusion usually die before arrival in the ED. Vital signs were within normal limits.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergencydepartment with chest pain. He was worked up non-emergently in the ED with pain recurring and resolving multiple times during his stay. EKG 1, 1646: What do you think?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content