This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. The ED activated trauma services, and a 12 Lead ECG was captured. The fall was not a mechanical etiology.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. The patient re-presented to the ED a few days after his discharge with syncope. Edited by Smith He also sent me this great case.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He called EMS who brought him to the ED. ED Diagnoses: 1. This history immediately places this patient in a high -prevalence population for having an acute event.
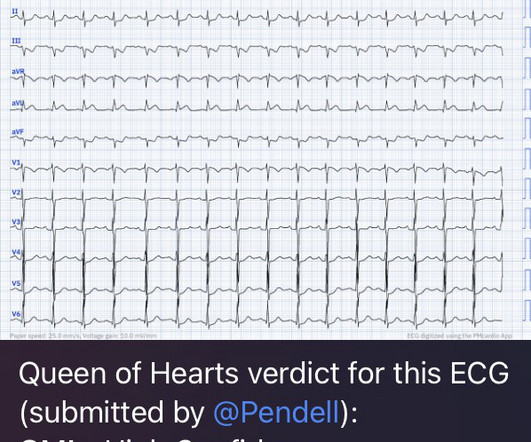
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
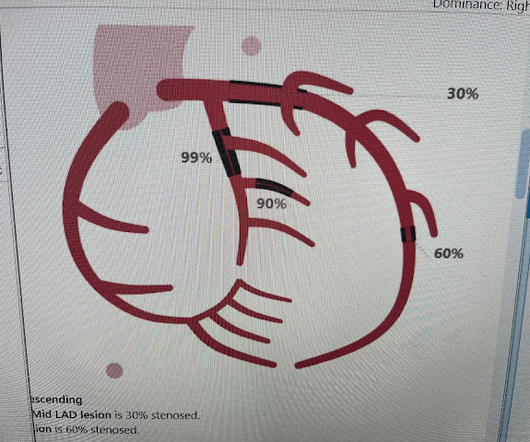
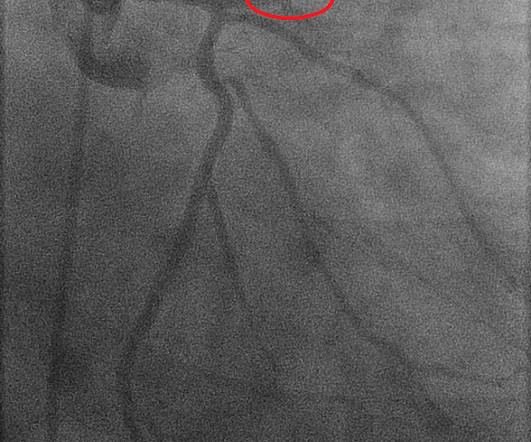
link] A 30 year-old woman was brought to the ED with chest pain. However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This is written by Brooks Walsh.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al. There is no further workup at this time.
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. Unfortunately — 1.5
Takotsubo is a sudden event, not one with crescendo angina. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD.
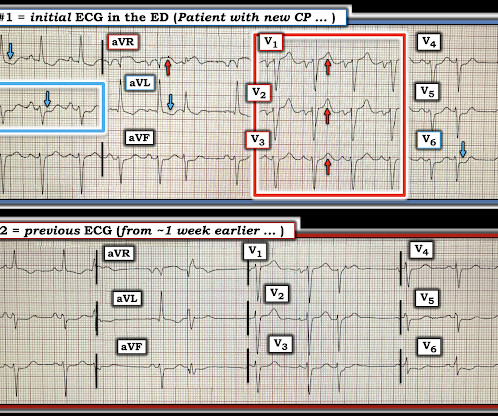
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. There is unfortunately no way to justify the sequence of events with resultant delay in diagnosis and treatment — and ultimate catastrophic infarction that rendered a previously healthy teenager a candidate for cardiac transplantation.
Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. He also had non-acute CAD of the RCA (50%) and LCX (50%). I focus my att ention on the interpretation of the initial ED tracing ( = E CG # 1 in Figure-1 ). It is not normal to see ≥1.5
CAD-RADS category 1. --No That said — I did not feel the history we were given pointed to any particular diagnosis ( ie, 3 episodes of CP and dyspnea of uncertain duration over the past day — with pain on deep breathing — but with symptoms apparently resolved by the time the patient arrived in the ED ).
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. Clinical Course: - He had no events on cardiac monitoring overnight. - Of interest Lead I on the initial ECG from the ED = ECG #2 ( which was done a bit after the prehospital ECG #1 was done ) no longer shows this unusual 4-phase QRS deflection in lead I.
She had zero CAD risk factors. Subsequent events: Later, before being taken to her room, the 2nd troponin returned at 1.01 The 1st “lesson” is, “All bets are off” — when an adult of any age presents to the ED with new-onset chest discomfort. hours of substernal chest pressure. Here was her ECG at time zero: What do you think?
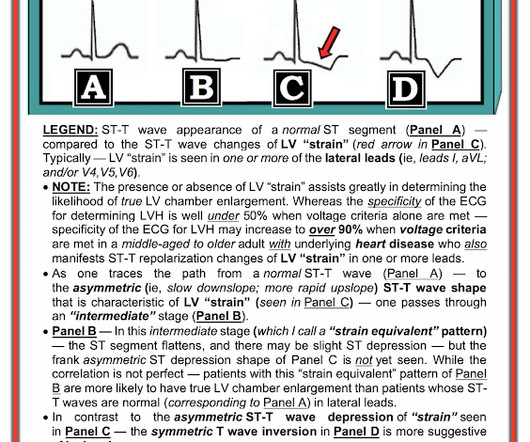
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. Electrocardiographic left ventricular hypertrophy in chest pain patients: Differentiation from acute coronary ischemic events. Is the ST elevation due to LVH? Her vitals signs were remarkable for marked hypertension.
She was asymptomatic at the time of this ECG recorded on arrival to our ED: What do you think? She also had non-acute CAD of the left main (50%) and LCX (75%). By the time the patient arrived at our facility, she had received aspirin and nitroglycerin, and her pain had apparently completely resolved. They opened it.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. Folland ED, et al. In the cath lab, the patient’s blood pressure remained low. De Backer D et al.
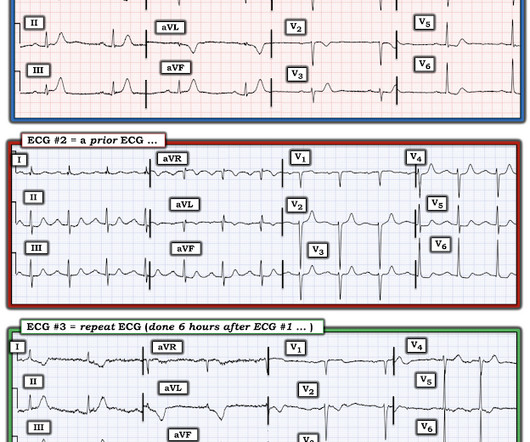
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. The Repeat ECG: As per Dr. McLaren — the patient was unfortunately discharged from the ED — but returned 6 hours later with a recurrence of chest pain.
He arrived at the ED just shy of two hours after onset, pain free. No prior similar symptoms or known CAD. This history immediately places this patient in a higher -risk category for having an acute cardiac event ( ie, meaning we need to rule out an acute event, rather than the other way around ).
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out."
This 60-year old woman clearly presented to the ED as a higher -risk patient given her history of known coronary disease, now with new chest pain. This was sent to me by a former resident who is outstanding at reading ECGs for OMI. "Hi Figure-1: Comparison between the first 2 ECGs in today's case.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He was worked up non-emergently in the ED with pain recurring and resolving multiple times during his stay. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content