This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
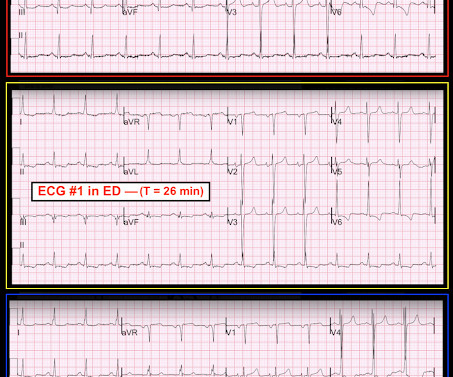
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
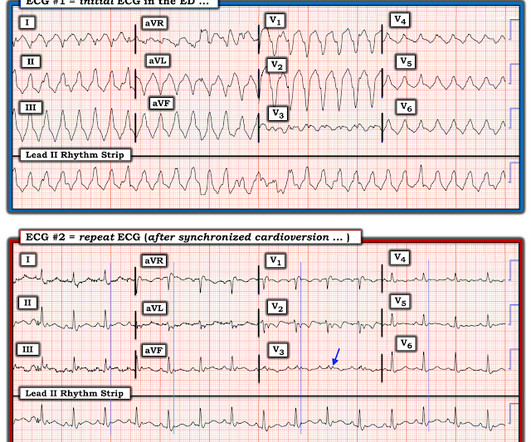
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He called EMS who brought him to the ED. ED Diagnoses: 1. We've come a long way in 2 years! And the pace only quickens. Epigastric pain 2.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Edited by Smith He also sent me this great case. The undergraduate's analysis: This EKG shows J point elevation of about 0.5-1
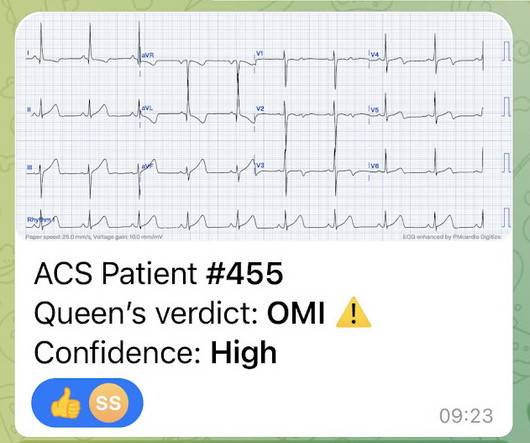
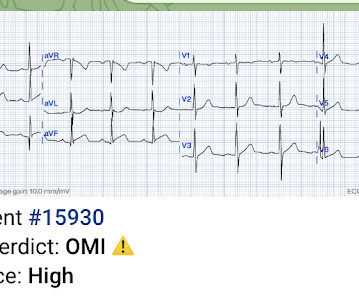
Here is what the Queen of Hearts AI app says: The patient received aspirin and NTG prehospital, and was transported to the ED. It could be a proximal RCA with both inferior OMI, posterior OMI (pulling ST down in V1/V2), and RV OMI causing large ischemic T-waves in V3-4.
Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. Background: Chest pain is one of the most common presentations to the ED. In prior decades nearly all patients presenting to EDs with chest pain were admitted to hospital. AEM June 2022.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chest pain associated with nausea/vomiting 30 min PTA. This was stented with a 2.25
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. Here is the final ECG just prior to ED transfer. Attached below is the initial ED tracing upon hospital arrival, approximately 25 minutes after the prehospital ECG. A 12 Lead ECG was recorded. No serial ECG’s were recorded.
The case An older woman presented to the ED with dyspnea, diaphoresis, and chest pressure. She had a normal EF, and no significant CAD, and was taking flecainide to suppress the AF. Wide-complex tachycardia: VT or aberrant, or "other?" This case is contributed by Brooks Walsh , an EM physician and ECG expert from Connecticut.
Their feedback represent ed over 957 incidents overall and provided a ton of information to help iron out some of the initial wrinkles. With API , participating CAD and RMS vendors will be able to automatically send data back and forth to NERIS. Here is a recap in case you were unable to attend or need a refresher. What is NERIS?
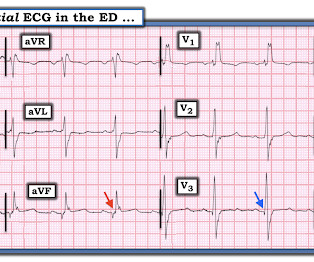
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. So I made an ED diagnosis of Non-Occlusion Myocardial Infarction (NOMI), and his next day angiogram confirmed NOMI. Figure-1: The initial ECG that was done in the ED ( See text ). Here is his initial ECG: What do you think?
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
link] A 30 year-old woman was brought to the ED with chest pain. However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This is written by Brooks Walsh.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
He had a history of CAD with CABG. Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. A middle-aged male had a V Fib arrest. He had not complained of any premonitory symptoms (which is very common). There is profound ST depression especially in I, II, V2-V6.
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. The ED provider ordered a coronary CT scan to assess the patient for CAD. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive. Another blood pressure was checked.
Diagnosis of MINOCA should be made according to the Fourth Universal Definition of MI, in the absence of obstructive coronary artery disease (CAD) (no lesion ≥50%). The authors recommend using optical coherence tomography or intravascular ultrasound imaging in patients with evidence of nonobstructive CAD by angiogram. The K was normal.
He had a family history of early CAD and occasional drug and tobacco use. The ECG was alarming to the ED physician who did indeed review it. An ECG is recorded and the computer reads it as "normal". Do you want to see it? Or would you rather not be bothered? I'd rather be bothered.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. He has a history of known CAD, diabetes, and dyslipidemia. The ED ECG in the context of the prehospital ECGs was indeed diagnostic of acute coronary occlusion. Leads II, III, aVF show about 0.5
CAD-RADS category 1. --No That said — I did not feel the history we were given pointed to any particular diagnosis ( ie, 3 episodes of CP and dyspnea of uncertain duration over the past day — with pain on deep breathing — but with symptoms apparently resolved by the time the patient arrived in the ED ).
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. He was diagnosed as NSTEMI.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. Pericarditis? . == MY Comment by K EN G RAUER, MD ( 12/13/2019 ): == I LOVE this post — as it explores the important decision-making process associated with the ED diagnosis of a cute P ericarditis. No acute culprit. He was admitted to cardiology.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. There was no prodrome and no associated symptoms such as SOB or CP. The medics recorded an ECG: There is STE in V1-V3 and aVL, with reciprocal ST depression in II, III, aVF. The medics were worried about STEMI, as it meets STEMI criteria. What do you think?
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergency department (ED). This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries.
A woman in her 60s with no prior history of CAD presented with 3 hours of sharp, centrally located chest pain with radiation to the anterior neck, with associated nausea. Medics recorded 2 ECGs, one before and one after sublingual NTG, and both are similar to the first ED ECG. Use ED Echo if available 4. Why did I say this?
Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. He also had non-acute CAD of the RCA (50%) and LCX (50%). I focus my att ention on the interpretation of the initial ED tracing ( = E CG # 1 in Figure-1 ).
She had zero CAD risk factors. Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 hours of substernal chest pressure. There is 1 mm of STE in lead V2.
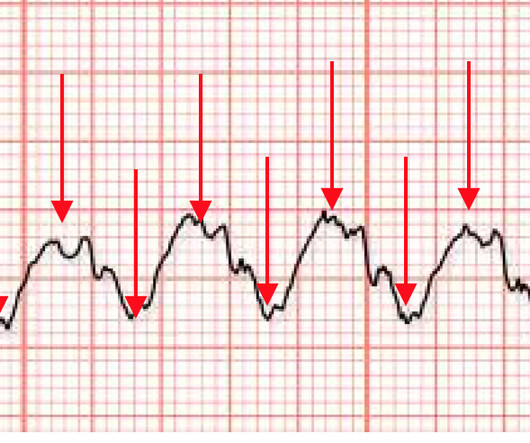
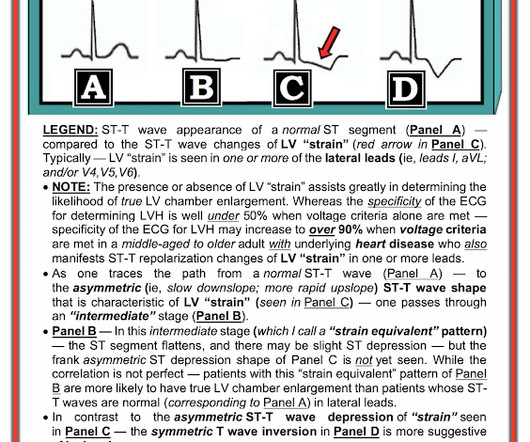
This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. See image below: Slow upstroke, fast downstroke. Asymmetric. NOTE: Any 1 or 2 of the above ECG findings in a patient with new CP would suffice to justify the need for prompt cath with PCI.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. V1 has 0.5 mm of elevation. ng/mL [IQR: 0.46, 2.35]. Learning Points: 1.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. In the cath lab, the patient’s blood pressure remained low.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. There is ST elevation, but also high voltage (though the high voltage is NOT in the leads with worrisome STE, rather, it is in aVL). Is the ST elevation due to LVH? Her vitals signs were remarkable for marked hypertension.
Despite otherwise normal vital signs, she was appropriately triaged to the critical care area of the ED. They are rare and hard to find in normal practice in the ED. She denied chest pain and denied feeling any palpitations, even during her triage ECG: What do you think? Or it could simply still be classic VT. RVEF 100 ml/m2.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED. He reported to EMS a medical history of GERD only. However, in this context (i.e. ST-elevation, etc.)
Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. The ST changes went overlooked by both the ED physician and the on-call cardiologist, and the patient was subsequently admitted to telemetry. There was no obvious pallor, diaphoresis, or dyspnea, and he denied any prior episodes of vomiting.
Cardiology refused to be the admitting physician because it was "NSTEMI", and forced the ED physician to admit the patient to the hospitalist. Of course, there was terrible boarding and the patient was considered non-emergent (NSTEMI), and so could not leave the ED for some time. Scattered other nonobstructive CAD.
Reyes LF, Garcia E, Ibáñez-Prada ED, et al. Included 584 patients > 18 years admitted to ICU with severe PNA based on IDSA/ATS criteria Primary Outcome: 60-day all-cause mortality Hydrocortisone 16% vs. placebo 18%, adjusted OR 0.90 (95% CI 0.57-1.40) 1.40) Trial likely underpowered.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 He denied chest pain or shortness of breath. See below for PM Cardio digitized version of this. There was a 0.9%
Patients were then were randomized to receive CTCA in the ED or “standard of care only” The primary outcome was, naturally, the glorious typical cardiology trial outcome of death or non-fatal myocardial infarction at one year. Other differences in medical or preventive management did not differ by study arm.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. In this study of dialysis patients with severe CAD, 77% had an abnormal resting EKG and the most common abnormality was LVH. Herzog et al.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content