This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Of course, writing “hypertensive emergency, underlying CAD with demand ischemia, or NSTEMI all remain on the differential” makes no sense.
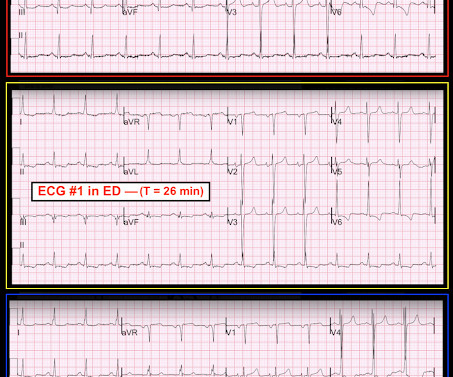
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. The ST changes went overlooked by both the ED physician and the on-call cardiologist, and the patient was subsequently admitted to telemetry. it has been subsequently deemed a STEMI-equivalent. However, when the Troponin I returned 8.4
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 There are hyperacute T-waves in V5 and V6. Next trop in AM.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He called EMS who brought him to the ED. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. Here is the final ECG just prior to ED transfer. A 12 Lead ECG was recorded. The pathology is now painfully evident.
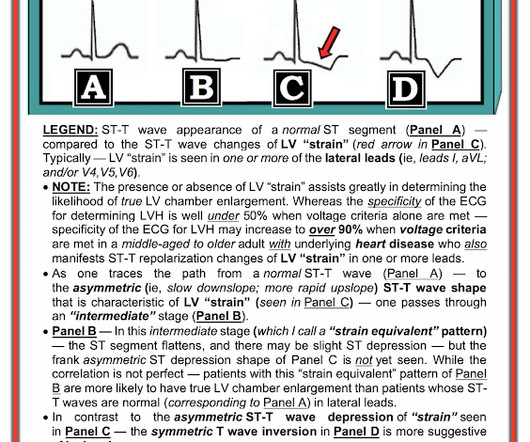
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
He had a history of CAD with CABG. Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. A middle-aged male had a V Fib arrest. He had not complained of any premonitory symptoms (which is very common).
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. The ED provider ordered a coronary CT scan to assess the patient for CAD. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive. Another blood pressure was checked.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Most recent echo showed EF of 60%.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic."
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
link] A 30 year-old woman was brought to the ED with chest pain. However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This is written by Brooks Walsh.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. He denied chest pain or shortness of breath.
This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI.
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergency department (ED). This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries.
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He had a family history of early CAD and occasional drug and tobacco use. The ECG was alarming to the ED physician who did indeed review it. Unknown algorithm Interpretation: Inferior ST elevation, with reciprocal ST depression in aVL.
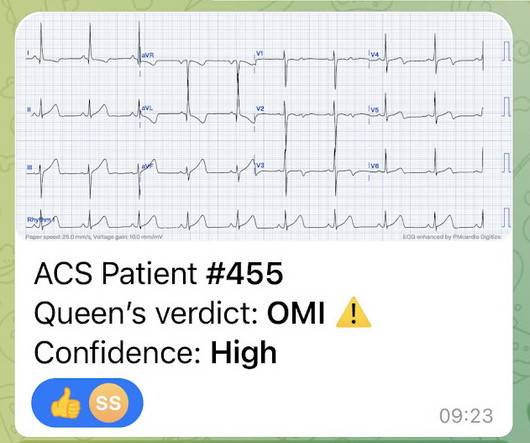
Since then, I started looking for OMI EKG findings and not just STEMI. Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Risk Factors: High Cholesterol.
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. He has a history of known CAD, diabetes, and dyslipidemia. The ED ECG in the context of the prehospital ECGs was indeed diagnostic of acute coronary occlusion. Leads II, III, aVF show about 0.5
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. This was my response: "This looks like a worrisome EKG. But by now you must have a repeat ECG.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery? Beware crescendo angina in patient with known CAD ST Elevation in aVR Case 7.
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? He also had non-acute CAD of the RCA (50%) and LCX (50%).
CAD-RADS category 1. --No Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The Transient STEMI is at high risk of re-occlusion.
Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. Some are STEMI-equivalents. Look at aVF.
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. I could have told you this (and did tell you this) without an MRI.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. The medics were worried about STEMI, as it meets STEMI criteria. The troponins are NOT consistent with STEMI (OMI), which typically has a troponin I of at least 5 ng/mL. There was no prodrome and no associated symptoms such as SOB or CP.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. Pericarditis?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. The value of Stat Echo in the ED for confirming clinical and ECG suspicion of acute PE cannot be overstated!
She had zero CAD risk factors. It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? A repeat ECG was performed and cardiology was re-consulted: Roughly unchanged. No acute culprit. Pericarditis?
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. 2 The astute paramedic recognized this possibility and announced a CODE STEMI.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. In this study of dialysis patients with severe CAD, 77% had an abnormal resting EKG and the most common abnormality was LVH. Herzog et al.
Cardiology refused to be the admitting physician because it was "NSTEMI", and forced the ED physician to admit the patient to the hospitalist. Of course, there was terrible boarding and the patient was considered non-emergent (NSTEMI), and so could not leave the ED for some time. Scattered other nonobstructive CAD.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Below is the ECG. Take home 1.
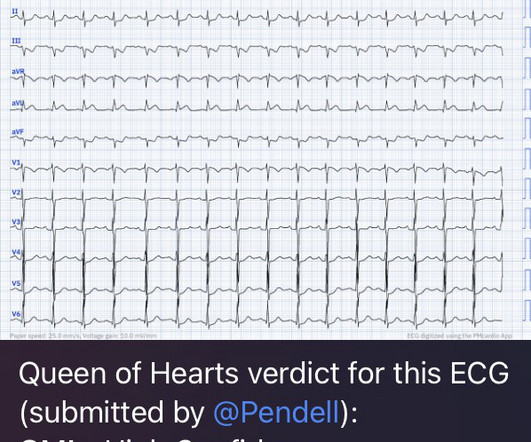
He arrived at the ED just shy of two hours after onset, pain free. No prior similar symptoms or known CAD. Here is the initial ED ECG: Here that first ECG is cleaned up by PM Cardio app: What do you think? The Queen of Hearts Diagnosed "STEMI/STEMI equivalent" on that first ECG (she now uses "STEMI Equivalent" rather than OMI).
The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. Pre-intervention. In other words, millimeters really don't matter!
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content