This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
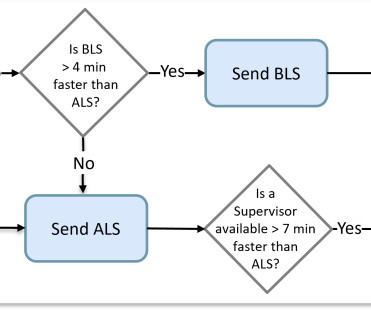
Dispatching the right unit to an EMS call was much simpler when all resources had the same capabilities and a response time was the primary measure of success. It was a matter of determining which crew was available closest to the scene.
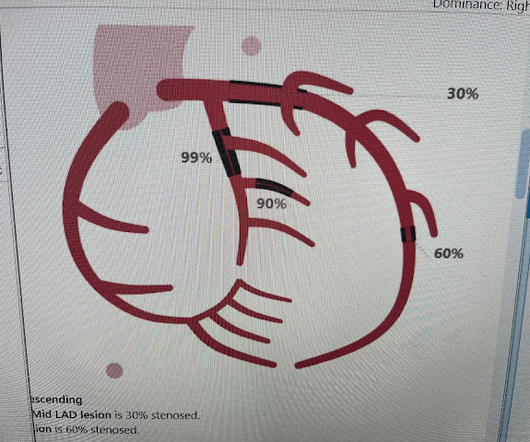
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. 2. Coronary angiography reveals significant and severe CAD involving all three epicardial vessels. His spouse had called 911 after she heard a loud “thud” in the adjacent room. He was taken to the Cath Lab.
Were making the jump to general availability (GA) and adding new features such as CAD and Cardiac Monitor integrations, Longitudinal Record (LR), and Mobile-to-Mobile functionality. This basic version will not include auto-import configuration, and integrations with CAD and EHR will not be added until upcoming releases in 2025.
WE, AS EMS PROFESSIONALS, SHALL PROVIDE COMPASSIONATE, APPROPRIATE CARE TO ALL PATIENTS. CAD notes indicate that the caller was walking in the park and came across a vehicle in the far corner of the parking lot. EMS must rely on the hazmat team to monitor the air and not rely on their sense of smell.
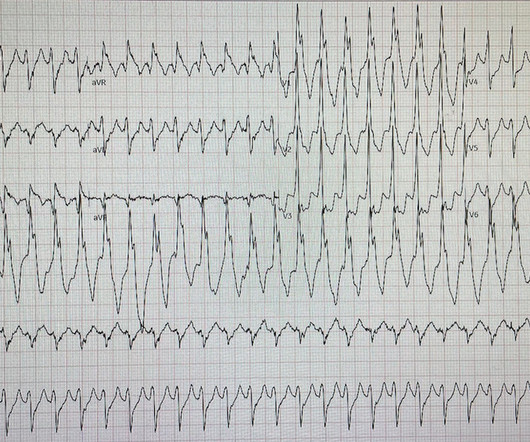
He denied any known history of CAD, but did report ASCVD risk factors to include HTN, HLD, and DM. David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. The patient was very uncomfortable, dyspneic, and displayed an SpO2 90% on RA.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
EMS personnel found him seated on a bench, uncomfortable, but without gross distress. Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. A third, and final, EMS 12 Lead ECG was recorded: The precordial ST segments (even Leads I/aVL, as well) have reverted to a dramatically depressed state.
He reported to EMS a medical history of GERD only. Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. However, in this context (i.e.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. He called EMS who brought him to the ED. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A 12 Lead ECG was recorded. A 12 Lead ECG was recorded.
His daughter immediately started CPR and another family member called EMS. When EMS arrived the patient was in ventricular fibrillation. Written by Willy Frick A man in his 50s was at home with his family when they heard a thud and rushed into the room to find him unconscious with agonal respirations.
However, in a data-driven world, it is imperative that fire and EMS organizations have timely and accurate information at their fingertips. Once the new system is in place, it will also be able to integrate information from the computer-aided dispatch system (CADS).
Investigators sought to evaluate responses by emergency medical services (EMS) at El Paso-Juárez ports of entry (POE). Methods: This cross-sectional, retrospective study evaluates prehospital care provided by EMS at three international bridges in El Paso. The busiest month was July, with a median of 132 encounters.
Your existing historical CAD records contain the necessary information to build such dynamic views in real-time. The existence of identifiable causes explains the ability to properly forecast the vicinity of calls in addition to their timing.
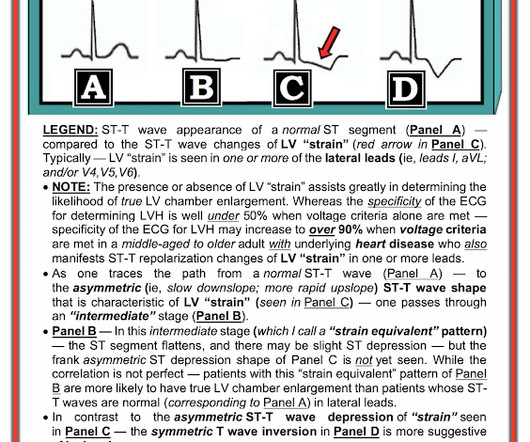
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. 1] European guidelines add "regardless of biomarkers".
These concerns were readily conveyed to my supervising cardiologist with particular emphasis on high pretest probability for baseline advanced CAD (3-vessel disease, specifically) with a critically stenosed proximal LAD. A quick way to validate this conjecture is to simply acquire a secondary ECG, but I failed to do this in the moment.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. A rectal temperature was obtained which read 107.9
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. He was diagnosed as NSTEMI.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow).
A middle-aged male with h/o CAD and stents presented with typical chest pressure. EMS recorded the following ECG: What do you see? Here is his ECG: The resident was alarmed at the "ST elevation in III with reciprocal ST depression in aVL" Are you alarmed? This is a very common misread. The trick is to find the end of the QRS.
If the EMS Gods knew better, they would never put us together as when we combine partnerships, we turn into a black cloud. We found the address matching that of a farm, but the message on our CAD (Computer Assisted Dispatch System) said the location was towards the back of the farm and in a trailer. Me: “Pretty quiet here.”
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. There is mild-moderate tricuspid valve regurgitation. Overall CMR findings are consistent with arrhythmogenic cardiomyopathy. RVEF 100 ml/m2.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. I could have told you this (and did tell you this) without an MRI.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. There is a limit to the amount of voltage that prehospital ECGs in most EMS systems are able to display. There was no prodrome and no associated symptoms such as SOB or CP. The medics were worried about STEMI, as it meets STEMI criteria. What do you think?
This case is contributed by Brooks Walsh , an EM physician and ECG expert from Connecticut. She had a normal EF, and no significant CAD, and was taking flecainide to suppress the AF. The case An older woman presented to the ED with dyspnea, diaphoresis, and chest pressure.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot.
EMS found the patient in VFib and performed ACLS for 26 minutes then obtained ROSC. The patient was transferred immediately for angiogram which revealed no significant CAD, and no intervention was performed. I do not see clear evidence of OMI or reperfusion at this time.
She also had non-acute CAD of the left main (50%) and LCX (75%). J of National Association of EMS Physicians 2014. Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. They opened it. Initial troponin T was 0.46 Ownbey et al.
One North American EMS system recently had 245 overdoses in a single day. During this engaging session, we will explore cutting-edge technology that EMS systems use to tackle this problem in near real-time. Identifying, tracking, and mapping overdoses is key to effective intervention.
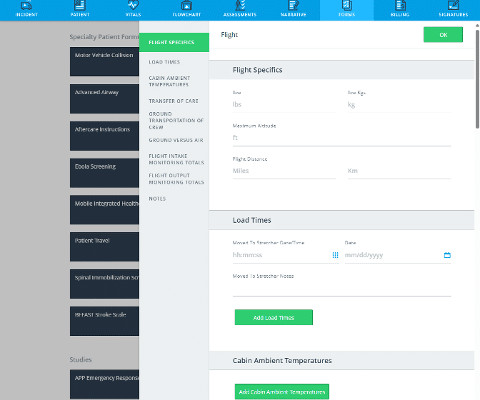
With this consideration, ESO will continue to partner with EMS agencies as you transform your roles beyond traditional EMS responses. Part of this will include expanding the Electronic Health Record (EHR) beyond the NEMSIS standard to allow for more flexibility in clinical documentation.
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. Academic EM. For this box, please keep ventricular tachycardia (VTach) and supraventricular tachycardia with aberrancy (SVT with aberrancy) in your differential. This EKG comes from a 75-year-old male presenting with palpitations. Take a look: Figure 3. Did you read it?
With FirstWatch , we are able to provide the number of calls on each bill, but we also include the date and time, report number, CAD number, jurisdiction, and other details for the recipient to review. If my EMS chief wants a report, I can send a dashboard that provides data, as well as some context, in almost no time.
Connections with CAD, Billing, and Patient Outcomes Seeing the full picture of a patient’s care is key, and new technology is making the response for prehospital care faster and more efficient than ever.
Improve resource allocation ESO EHR is fully interoperable, connecting to computer aided dispatch (CAD), Cardiac Monitors, Billing, and pre-hospital and hospital systems, so you can transfer patient care data across mobile applications. Why do these updates matter?
These ECGs were texted to me by one of our previous ultrasound fellows, Will Smoot An elderly male arrived via EMS for acute substernal chest pain with radiation to left shoulder and arm that awakened him from sleep at 0030. He took two full strength aspirin prior to EMS arrival. No prior similar symptoms or known CAD.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content