This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. Given no clinical prelude of anginal (or equivalent) descriptors, prior to the acute event, risk stratification of the ECG and Troponin was pursued via Echo and nuclear Myocardial Perfusion Imaging (MPI).
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. This history immediately places this patient in a high -prevalence population for having an acute event. This is a re-post of an excellent case from 2021. Respect physiology.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. Of course, writing “hypertensive emergency, underlying CAD with demand ischemia, or NSTEMI all remain on the differential” makes no sense.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. AEM June 2022.
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. Adverse events are common in those using GLP-1 agonists, but the vast majority of these are minor. Take for example semaglutide.
No one can tell you who will be that very next person to dial 9-1-1; however, it is imperative for the effectiveness of deployment that we concede that people and events often follow certain predictable patterns. Your existing historical CAD records contain the necessary information to build such dynamic views in real-time.
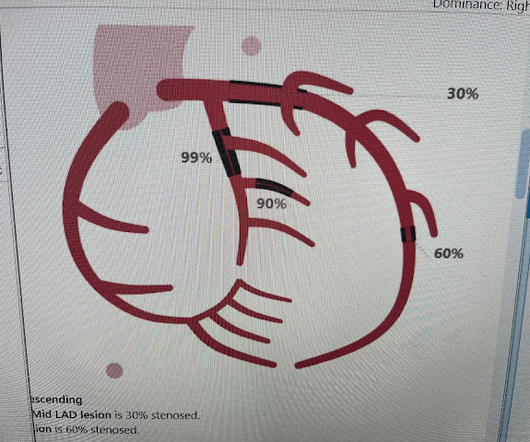
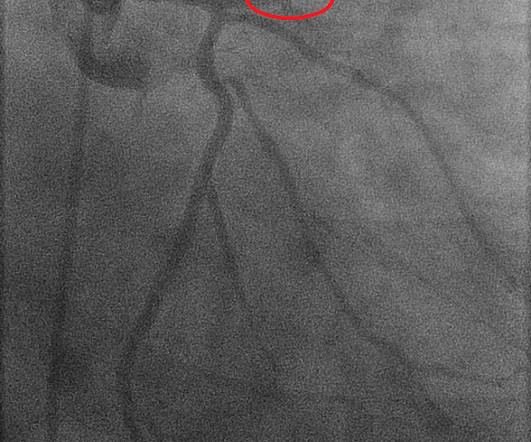
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. Angiography Angiography was performed after aspirin and heparin were started.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
Takotsubo is a sudden event, not one with crescendo angina. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. V1 has 0.5
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. He was diagnosed as NSTEMI.
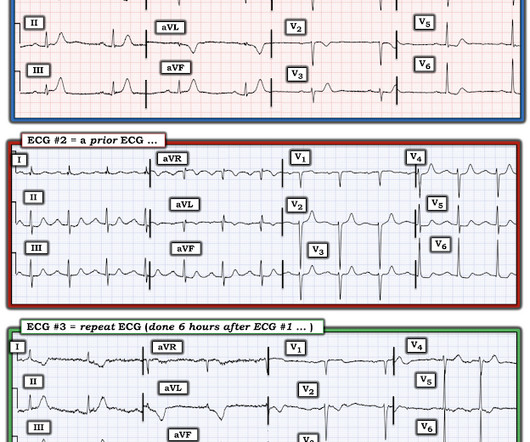
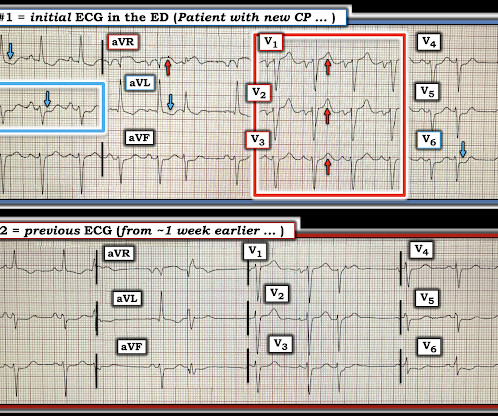
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The pain initially started the day prior to presentation.
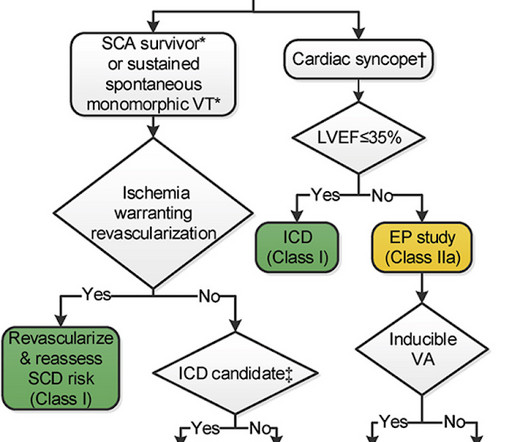
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. Clinical Course: - He had no events on cardiac monitoring overnight. - There was no prodrome and no associated symptoms such as SOB or CP. The medics recorded an ECG: There is STE in V1-V3 and aVL, with reciprocal ST depression in II, III, aVF. What do you think?
CAD-RADS category 1. --No At this point, with the information above, the patient's overall clinical picture could be consistent with either reperfused OMI, or Non-OMI, since both may have absent pain and inverted T waves. A repeat troponin returned at 0.45 ng/mL, consistent with reperfused OMI, or Non-OMI. A CT Coronary angiogram was ordered.
She had zero CAD risk factors. Subsequent events: Later, before being taken to her room, the 2nd troponin returned at 1.01 hours of substernal chest pressure. It was non-radiating and without other associated symptoms except for nausea. Here was her ECG at time zero: What do you think? There is ST elevation in V2 with large fat T-wave.
The patient was transferred immediately for angiogram which revealed no significant CAD, and no intervention was performed. All of these episodes occurred without any symptoms reported from the patient, even after pointed questioning during the telemetry events. I do not see clear evidence of OMI or reperfusion at this time.
He also had non-acute CAD of the RCA (50%) and LCX (50%). Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. 100% proximal LAD thrombotic occlusion with TIMI 0 flow was found and stented with excellent angiographic result and TIMI 3 flow.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. There is ST elevation, but also high voltage (though the high voltage is NOT in the leads with worrisome STE, rather, it is in aVL). Is the ST elevation due to LVH? Her vitals signs were remarkable for marked hypertension.
As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
CAD notes indicate that the caller was walking in the park and came across a vehicle in the far corner of the parking lot. TRIGGER WARNING: TOPICS OF SUICIDE MAY BE HARD FOR SOME PEOPLE TO READ ABOUT. THIS ARTICLE IS COVERING THE MEDICAL ASPECTS OF CHEMICAL SUICIDES. Its mid-Monday morning on a crisp spring day.
Stated differently, the differential diagnosis for the presenting syndrome was either ventricular fibrillation due to acute coronary syndrome, or idiopathic ventricular fibrillation and bystander stable CAD. As per Dr. Frick — "Angiography can be misleading — and must always be understood in clinical context".
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chest pain or shortness of breath. PM Cardio digitized version.
This case represents the same physiologic event as OMI in terms of the result on the myocardium, therefore with identical ECG features, however there may not be ACS! Therefore this patient is either in some form of SVT or atrial flutter. Atrial flutter, when regular, must be conducting at 1:1, 2:1, 3:1, etc. Clear lungs. Perfused extremities.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island. I remember Allie well from her days in the Research volunteer program at Hennepin. F (rectal). There was a 0.9%
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. Below is the ECG. What do you think? There’s sinus bradycardia, first degree AV block, normal axis, delayed R wave progression, and normal voltages.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. No similar symptoms in the past. No prior exertional complaints of chest pain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. No further troponins were measured. Pericarditis?
I C Blood samples Management Recommendation Level of evidence Serum biomarkers of myocardial infarction ( troponin ) should be sampled as early as possible without delaying reperfusion therapy. I C Symptom relief Symptom Management Recommendation Level of evidence Hypoxia Oxygen is indicated if SaO2 < 90% or PaO2 < 60 mmHg.
She also had non-acute CAD of the left main (50%) and LCX (75%). Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Initial troponin T was 0.46
No prior similar symptoms or known CAD. This history immediately places this patient in a higher -risk category for having an acute cardiac event ( ie, meaning we need to rule out an acute event, rather than the other way around ). He arrived at the ED just shy of two hours after onset, pain free. ng/L) -- slightly elevated.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. He said it felt like "someone ripped [his] heart out."
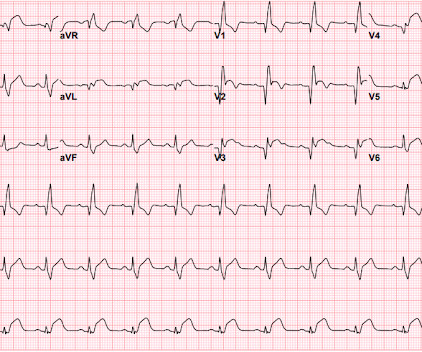
Hi Steve wonder what you think of this ecg in a 60 yo woman w cp, known CAD" Presentation ECG (ECG 1): Here is her previous from one week prior when she presented with heart failure and trops were "negative" (ECG 2): My response: "They both look like active ischemia. He did not get a repeat ECG after the NTG.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. It may or may not represent early findings in a new acute event. Also : See Ken Grauer's excellent comments at the bottom. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content