This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
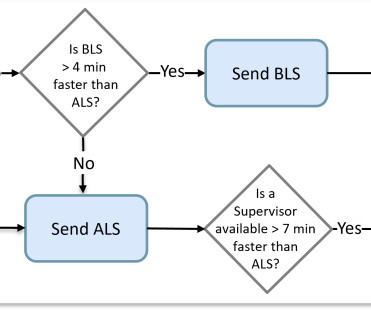
Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance. Today, we have many more decision constraints that complicate the assignment process.
Were making the jump to general availability (GA) and adding new features such as CAD and Cardiac Monitor integrations, Longitudinal Record (LR), and Mobile-to-Mobile functionality. This basic version will not include auto-import configuration, and integrations with CAD and EHR will not be added until upcoming releases in 2025.
CAD notes indicate that the caller was walking in the park and came across a vehicle in the far corner of the parking lot. The ability to mix and match chemicals that are toxic and/or fatal is expansive, and in todays information age, its unfortunately at everyones fingertips. Chemical Assisted Suicide: Reponder Information.
However, in a data-driven world, it is imperative that fire and EMS organizations have timely and accurate information at their fingertips. This information allows fire departments to properly allocate resources, understand their community’s risk, and assess the performance of response units.
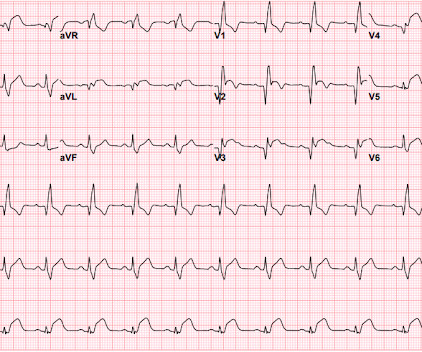
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System.
The National Emergency Response Information System (NERIS) is on track! F ire A dministration hosted their fourth informational webinar , NERIS Next Steps: Beta Launch, API Development, and Secondary Schema Release , to update departments on the current progress with NERIS and the anticipated timeline over the next three years.
In 2002, Jennifer transitioned to the Broomfield Police Department in Colorado where she dispatched and served as an Emergency Medical Coordinator, Communications Training Officer, Public Education Coordinator, and Computer-Aided Dispatch (CAD) Project Lead.
As fire departments prepare for the transition to the National Emergency Reporting Information System (NERIS), we understand there are many questions about how this new standard will fit into your operations. We will update and add new information as it becomes available, so be sure to bookmark this page and check back if questions arise.
Your existing historical CAD records contain the necessary information to build such dynamic views in real-time. The following animation demonstrates several spatial demand forecasts in quick succession that are normally separated in the real world by hours.
Police Department needs to keep informed in order to keep his community and officers safe. “If With FirstWatch, I get alerted through CAD triggers on my phone as soon as that call comes through. Having instant access to CAD data allows me to do this.” Lay of the Land It’s not just the CAD data the chief appreciates. “I
CT can provide important information. Considerations: Observational, many excluded, 2/3 of SDCT not scanned, adjudication of primary endpoint, patient centered outcomes not the primary outcome Key questions: When, Where, Type of CT and CCTA? Consider CT on the way up to the ICU once stabilized.
The National Emergency Response Information System (NERIS) is set to replace NFIRS by Q1 of 2025 – marking the biggest change to emergency response standard in the last 50 years. Department of Homeland Security, the Fire Safety Research Institute, and USFA hosted an informational webinar – Modernizing the U.S.
I hop into the ambulance, and log onto the CAD (Computer Assisted Dispatch) device. The call pops up onto our CAD. I look at the notes on the CAD it read: Crowning. I gather a few more pertinent information from dad regarding the mother’s pregnancy, it seems that everything has been going well for her. Me: “99 Fox.”
Fire Incidents | NERIS NFIRS, the current fire incident reporting system is being replaced by NERIS (National Emergency Response Information System) by the end of 2025. This toggle allows you to quickly and efficiently populate the Construction tab of the Occupant with the same information from the Building when necessary.
However, after all of that, even with the added information provided by CTCA, there was no difference in mortality or non-fatal myocardial infarction at one year. CTCA certainly has a role in the evaluation of patients with chest pain and possible CAD, but certainly not as a routine investigation in the ED. vs 60.8%.
Echocardiography can also provide meaningful prognostic information about diastolic function, severity of hypertrophy, chamber size, and valvular abnormalities. Objective information about functional capacity can be obtained from metabolic (cardiopulmonary) exercise testing.
The ED provider ordered a coronary CT scan to assess the patient for CAD. As a result — I always spend an extra brief moment comparing the digitized version to the original tracing to ensure all essential information is reliably transmitted. Another blood pressure was checked.
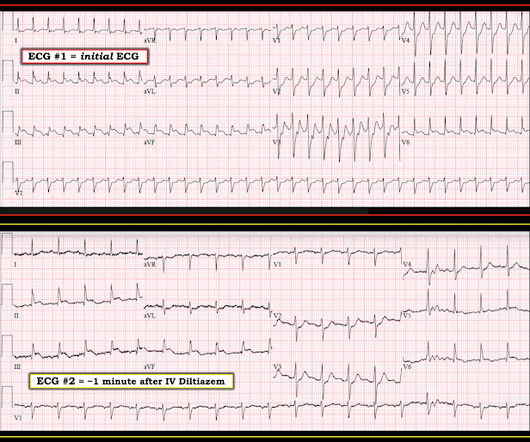
This new information makes the diagnosis of atrial flutter far more likely: first, atrial fibrillation and flutter are closely associated and, second, this makes a flutter rate of 200 bpm (with 1:1 conduction) quite likely. So we asked the patient if he had any new medications recently. He said, "I just started taking flecainide last week."
At this point, with the information above, the patient's overall clinical picture could be consistent with either reperfused OMI, or Non-OMI, since both may have absent pain and inverted T waves. CAD-RADS category 1. --No Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. There is 1 mm of ST elevation at the J-point in leads V2 and V3.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow).
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. This was sent to me with no information and I immediately replied that it was diagnostic of LAD OMI. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chest pain.
I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant." They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. Our THANKS to Dr. Meyers for presenting this informative case! No acute culprit. He was admitted to cardiology.
Meyers : This ECG was texted to me with no clinical information, and my response was: "That looks like a very subtle LAD OMI. He also had non-acute CAD of the RCA (50%) and LCX (50%). Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes.
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. I could have told you this (and did tell you this) without an MRI.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The pain initially started the day prior to presentation. Lead aVL, for example, has a definite J-wave.
She had zero CAD risk factors. I saw this before any other information and knew immediately that it represented an LAD occlusion. It was non-radiating and without other associated symptoms except for nausea. Here was her ECG at time zero: What do you think? There is ST elevation in V2 with large fat T-wave.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. Below is the ECG. What do you think? There’s sinus bradycardia, first degree AV block, normal axis, delayed R wave progression, and normal voltages.
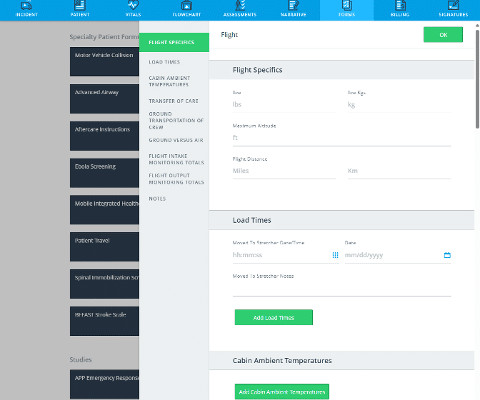
Here are a few highlights of how this new functionality can support your care delivery: Specific Workflows for Critical Care Documentation Documenting patient information in fast-paced situations, as well as long-term and complex transports, can be time-consuming. Interested in seeing the Critical Care capabilities (and more!)
Improve resource allocation ESO EHR is fully interoperable, connecting to computer aided dispatch (CAD), Cardiac Monitors, Billing, and pre-hospital and hospital systems, so you can transfer patient care data across mobile applications. Todays patient-centric care relies on connected information across each stage of a patients experience.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He looked back in time in the patient's chart and saw these ECGs and immediately recognized that they manifested subtle OMI. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content