This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 There are hyperacute T-waves in V5 and V6. Next trop in AM.
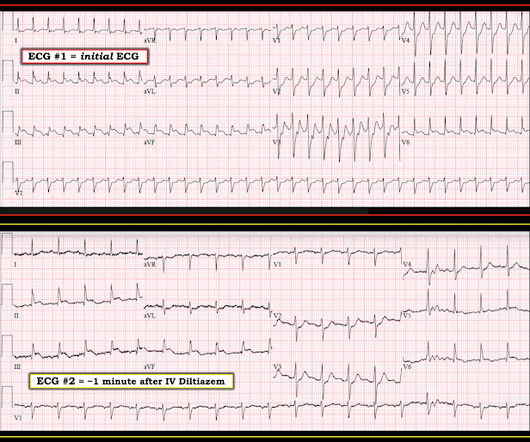
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. His ECG was repeated at this point: This shows a well developed anterior STEMI. The peak troponin I was over 100.
The ED provider ordered a coronary CT scan to assess the patient for CAD. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!)
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? So we asked the patient if he had any new medications recently. He said, "I just started taking flecainide last week."
At this point, with the information above, the patient's overall clinical picture could be consistent with either reperfused OMI, or Non-OMI, since both may have absent pain and inverted T waves. CAD-RADS category 1. --No Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. Pericarditis?
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. I could have told you this (and did tell you this) without an MRI.
Meyers : This ECG was texted to me with no clinical information, and my response was: "That looks like a very subtle LAD OMI. He also had non-acute CAD of the RCA (50%) and LCX (50%). Learning Points: Not all OMI will present as STEMIs. Sometimes serial ECGs minimizes the delay. Cath images: Before intervention.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). He had multiple cardiac arrests with ROSC regained each time.
She had zero CAD risk factors. I saw this before any other information and knew immediately that it represented an LAD occlusion. It is equivalent to a transient STEMI. It was non-radiating and without other associated symptoms except for nausea. Here was her ECG at time zero: What do you think?
I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant." They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. Our THANKS to Dr. Meyers for presenting this informative case! No acute culprit. He was admitted to cardiology.
Written by Jesse McLaren, with comments from Smith An 85 year old with a history of CAD presented with 3 hours of chest pain that feels like heartburn but that radiates to the left arm. There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Below is the ECG. Take home 1.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content