This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
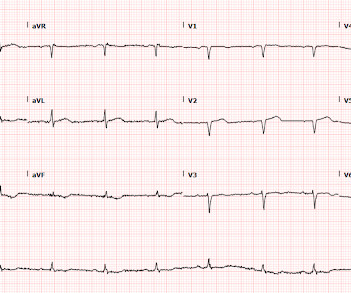
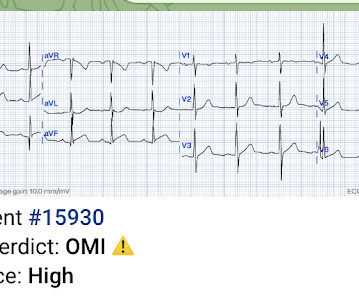
Patient 2 A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. He was discharged home.
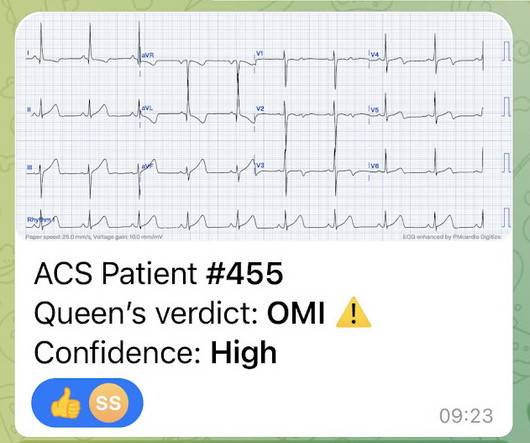
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. We've come a long way in 2 years!
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. Edited by Smith He also sent me this great case. The patient was put on a nitroglycerin drip and his pain improved with his blood pressure.
Otherwise, no admission of CAD, HLD, or family history of sudden cardiac death. link] deWinter first reported his unique characteristics of LAD occlusion in 2008, and since the respective ECG changes do not fit the conventional STEMI paradigm (as he even stated – “instead of signature ST-segment elevation” ….)
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 She reports associated SOB but no dizziness or LOC.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. His vital signs were unremarkable, and the lung fields were free of fluid congestion during auscultation.
He had no previous history of CAD, and presented with very typical waxing and waning chest pain, much worse with exertion but also present at rest and on presentation, though his pain was minimal at the time of the ECG. This is all suggestive of posterior STEMI, but not definitely diagnostic. I saw this 59 year old male 3 weeks ago.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Most recent echo showed EF of 60%.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I C Pain Titrated i.v. IIa C Anxiety Tranquillizer (e.g benzodiazepine) is considered.
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. PM Cardio digitized version.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic."
20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. Patient stated that he has had glucose over 400 even though he has not missed any doses of insulin. The ST depression vector includes these leads and cancels out the STE of the inferior OMI.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
He had a history of CAD with CABG. We found that 38% of out of hospital ventricular fibrillation was due to STEMI. Correlation of STEMI in Resuscitated Non-traumatic out-of-hospital Cardiopulmonary Arrest patients with Initial Rhythm and Cardiac Catheterization Findings (Abstract 580). A middle-aged male had a V Fib arrest.
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. A recent study found that SCAD causes almost 20% of STEMI in young women.
The ED provider ordered a coronary CT scan to assess the patient for CAD. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!)
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
So I went to look at the chart and here is the history: This patient with no h/o CAD had a couple of episodes of chest pain during the day, then presented with one hour of substernal chest pain that had some reproducibility but also improved from 10/10 to 5/10 with nitroglycerine. He was admitted to the hospital for a "rule out."
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He had a family history of early CAD and occasional drug and tobacco use. He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. Do you want to see it?
Concerning history, known CAD" Recorded 2 hours after pain onset: What do you think? The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. This was my response: "This looks like a worrisome EKG. But by now you must have a repeat ECG.
This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries. Figure 1: EKG for Dextrocardia showing STEMI. The second EKG was concerning for STEMI in the precordial leads (see figure 1). Click to enlarge.) 1 It has a prevalence of 0.01
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
As the pregnant population continues to age and with RF and smoking and DM still common we can expect to see pregnant woman with CAD. While interesting and exam worthy you’re still going to see STEMI on the ECH and have to go to the cath lab so perhaps it doesn’t change much of what we do. Improved care of complex.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
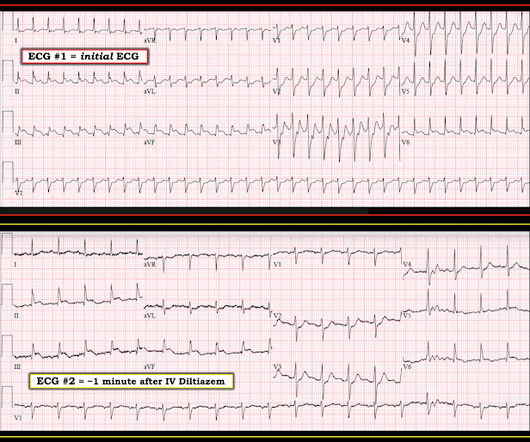
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Therefore this patient is either in some form of SVT or atrial flutter. If I fix the rhythm will the ST changes resolve? Clear lungs.
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. V1 has 0.5 mm of elevation. ng/mL [IQR: 0.46, 2.35]. Learning Points: 1.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. F (rectal).
He has a history of known CAD, diabetes, and dyslipidemia. The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. Moreover, T-wave inversion in aVL was also found to be 100% sensitive and 86% specific for inferior STEMI.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. 50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. Covid PCR negative.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. The medics were worried about STEMI, as it meets STEMI criteria. The troponins are NOT consistent with STEMI (OMI), which typically has a troponin I of at least 5 ng/mL. There was no prodrome and no associated symptoms such as SOB or CP.
CAD-RADS category 1. --No Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The Transient STEMI is at high risk of re-occlusion.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria.
Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. Some are STEMI-equivalents.
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? He also had non-acute CAD of the RCA (50%) and LCX (50%).
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. He was diagnosed as NSTEMI.
She had zero CAD risk factors. It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). There is also STD in V2-V4 (but maximal in V5-V6).
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. What do you see?
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? A repeat ECG was performed and cardiology was re-consulted: Roughly unchanged. No acute culprit. Pericarditis?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content