This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Help Support EM Cases by Giving a Donation here: [link] The post EM Quick Hits 59 Traumatic Coronary Artery Dissection, Proper Use of Insulin, Mesenteric Ischemia, Exercise Associated Hyponatremia, AI for OMI appeared first on Emergency Medicine Cases.
Jesse McLaren on when to consider Spontaneous Coronary Artery Dissection (SCAD), which patients are at risk for reocclusion, and the challenges of diagnosing SCAD in patients who have nonischemic ECGs despite silent occlusion, occlusions perfused by collaterals, or from non-occlusive MI on this ECG Cases.
Which had a coronary occlusion, and how acute were they? The post ECG Cases 25: ‘Late STEMI’ – How acute is the coronary occlusion? In this ECG Cases blog we look at 10 patients with potentially ischemic symptoms. appeared first on Emergency Medicine Cases.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
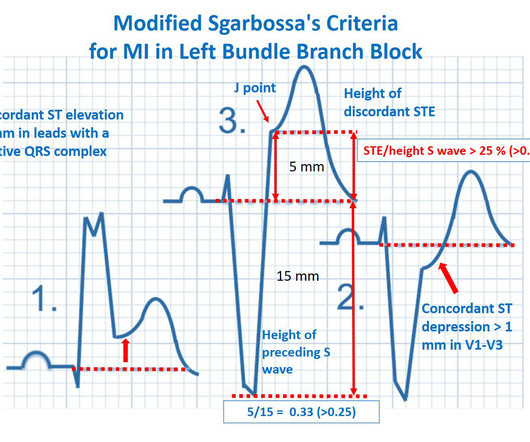
REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion Click here for Direct Download of the Podcast Modified Sgarbossa Criteria deWinters ECG Wellens’ Syndrome STEMI Criteria (Taming of the SRU) Resources REBEL EM: Modified Sgarbossa Criteria: Ready for Primetime?
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. As was emphasized by Dr.
Jesse MacLaren guides us through 10 cases of patients who present with generalized weakness or acute neurologic symptoms and discusses how to look for ECG signs of dysrhythmias, electrolyte emergencies, acute coronary occlusion, and demand ischemia in patients with generalized weakness and in patients with neurologic symptoms, to consider predisposing (..)
A 12-lead electrocardiogram (ECG) demonstrates ST elevations in leads II, III, and aVF with ST depressions in leads I and aVL and the team begins transport to the nearest percutaneous coronary intervention (PCI) capable hospital. Background: We have covered the issue of heart attacks several times on the SGEM. Reference: Stopyra et al.
FOAMed The post JC: Systematic review of the Manchester Acute Coronary Scores. St.Emlyn's - Emergency Medicine #FOAMed Journal Club on the impact of the MACS score in emergency medicine (systematic review). Learn how this tool improves diagnosis and patient outcomes while optimising hospital resources."FOAMed
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. The patient has no previous stress testing or coronary angiogram, and he is not low risk by HEART or EDACS scoring.
Myocardial infarction with non-obstructive coronary arteries: what is the prognosis? Giampaolo Niccoli1,2 and Paolo G. Camici3* 1Universita’ Cattolica del Sacro … Continue reading →
There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronary artery disease. 2. Coronary angiography reveals significant and severe CAD involving all three epicardial vessels. Strongly positive stress ECG Lexiscan administration. He was taken to the Cath Lab.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? He has no history of coronary artery disease. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. AEM June 2022.
Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Finally, do a coronary angiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. Coronary Angiography No angiographic significant obstructive disease.
ST/T changes: consider the differential including demand ischemia, associated electrolyte abnormalities, Brugada pattern from sodium channel blockade, and acute coronary occlusion vs vasospasm from cocaine. The post ECG Cases 47 – ECG Interpretation in Toxicology appeared first on Emergency Medicine Cases.
Isolated posterior MI is less common (3-8% of OMI) and presents with isolated ST-depressions in the anterior precordial leads (V1-V4), representing reciprocal changes to posterior left ventricular wall myocardial infarction as a result of distal occlusion of either the left circumflex or right coronary artery.
Why Was Cardiac Cath Negative for Coronary Disease? As noted by Dr. Nossen — this patient qualified as MINOCA ( M yocardial I nfarction with N on- O bstructive C oronary A rteries ) — since troponin was positive on his 2nd admission, yet there was no evidence of obstructive coronary disease on cath.
In this month's EM Quick Hits podcast: Megan Landes on the importance of diagnosing HIV in the ED, Jesse McLaren on the failed paradigm of STEMI criteria and ECG tips to identify acute coronary occlusion, Anand Swaminathan on evidence for non-invasive airway management in the poisoned patient, Brit Long and Hans Rosenberg on the identification, workup (..)
Question and Methods: The authors completed preplanned subgroup analyses to determine if a 0-1 hour ultra-sensitive troponin […] The post Sensitivity Cardiac Troponin T Among Patients With Known Coronary Artery Disease appeared first on EMOttawa Blog.
FOAMed The post Systematic review of the Manchester Acute Coronary Scores. St.Emlyn's - Emergency Medicine #FOAMed Journal Club on the impact of the MACS score in emergency medicine (systematic review). Learn how this tool improves diagnosis and patient outcomes while optimising hospital resources."FOAMed
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
The acute coronary syndrome work-up is negative but she is Well’s high and needs a CTPA to rule-out a pulmonary embolism. Lauren is currently funded by an NHLBI K12 grant (1K12HL138049-01) studying the implementation of evidence-based diagnosis of pulmonary embolism in the emergency department. Case: A 64-year-old woman with type-2 diabetes.
The Case A 62-year-old male with a history of Hypertension, Hyperlipidemia, Coronary Artery Disease with stents, Pulmonary Embolism on Eliquis, presents with sudden onset, severe, mid-sternal chest pain that started 15 minutes prior to arrival. Discussion Case Discussion: The patient’s history was concerning for an acute coronary syndrome.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection. Case: You are working a busy shift in a rural emergency department (ED) and your excellent Family Medicine trainee presents a case of a 63-year-old woman with chest pain and some intermittent radiation into the inter-scapular region.
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! It also does not uniformly indicate severe coronary disease. And what do you want to do?
Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. Design: Prospective, observational, before and after implementation of a protocol study. Known cardiac defibrillator. Pre-existing DNR order.
Risk factors that increase the likelihood of VT include history of previous myocardial infarction, known coronary artery disease, and structural heart disease. Increased age is also an independent risk factor for increased likelihood of VT in wide complex tachycardia. When in doubt, treat as ventricular tachycardia.
Coronary thrombosis is a dynamic process of platelet aggregation and subsequent coagulation. During spontaneous reperfusion -- whether via thrombolysis, or recruitment of collateral circulation -- there exists characteristic ST/T changes on the ECG. Case Review: [link]
She thinks she may have had stenting to her coronaries but … A 52 year old woman is triaged as a category 2 after complaining of chest tightness on the background of having previous cardiac history.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. It is spread to V2 and V3. References Naidu, S.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chest pain. As per Dr. Smith — today's patient is a 40-something year old patient with severe diabetes, renal failure and known coronary disease — who presents with “acute crushing CP”. Here is his ED ECG: What do you think?
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Reference: Wang et al.
Can you identify which ones had acute coronary occlusion? In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. The post ECG Cases 3: Can you find the subtle inferior MI? appeared first on Emergency Medicine Cases.
Which had acute coronary occlusion? In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI. The post ECG Cases 4: Lateral STEMI or Occlusion MI?
Which had acute coronary occlusion? 10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog. The post ECG cases 7: ST elevation in aVR, STEMI-equivalent?
Which patients with ECG evidence of coronary occlusion require a CT scan to rule out aortic dissection? What are the range of ECG findings in acute aortic dissection and how do they change management? Dr. Jesse McLaren guides us through 9 cases to answer these and other questions on ECG interpretation in aortic dissection.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. A Bayesian approach to acute coronary occlusion.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). This patient is actively dying from a left main coronary artery OMI and cardiac arrest from VT/VF or PEA is imminent!
Which had an acute coronary occlusion? Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves. In this ECG Cases blog we look at 6 patients who presented with potentially ischemic symptoms and LVH on their ECG.
Isolated posterior MI is less common (3-8% of OMI) and presents with isolated ST-depressions in the anterior precordial leads (V1-V4), representing reciprocal changes to posterior left ventricular wall myocardial infarction as a result of distal occlusion of either the left circumflex or right coronary artery.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content