This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
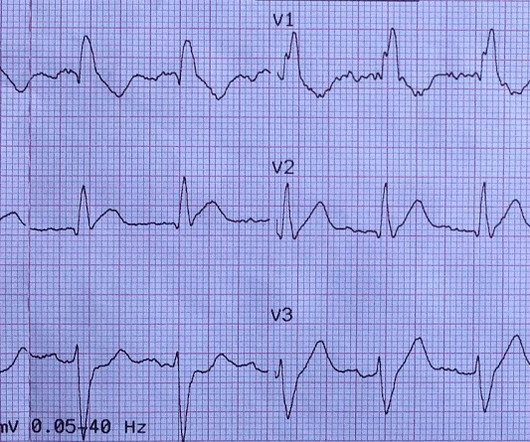
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
They started CPR. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! It also does not uniformly indicate severe coronary disease. He was defibrillated into VT.
The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. EMS arrives and finds the patient in monomorphic ventricular tachycardic (VT) cardiac arrest.
Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. Bystander CPR, a known predictor of good outcomes, was more common in the SDCT cohort than in the standard care cohort.
Did they get bystander CPR? Control: 53.4% D ECLS: 18.2% Control 8.7% Control 38.0% Majority of patients had PCI performed (96.6%) Impella CP was most common mechanical circulatory support in patients without ECLS (85.7%) Death From Any Cause at 30d ECLS: 47.8% Control: 49.0% RR 0.98; 95% CI 0.80 to 1.19; p = 0.81 Control: 9.6% Control 3.8%
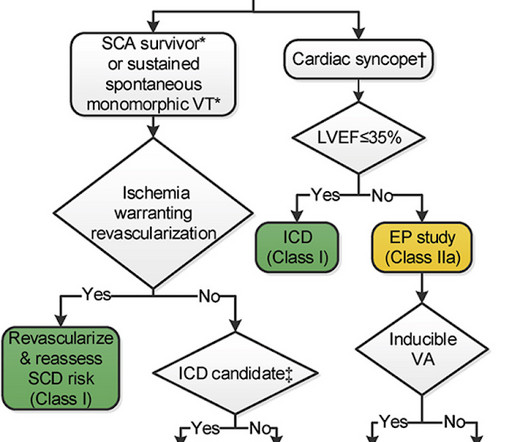
Emergent coronary angiography is not recommended over a delayed or selective strategy in patients with ROSC after cardiac arrest in the absence of ST-segment elevation, shock, electrical instability, signs of significant myocardial damage, and ongoing ischemia (Level 3: no benefit). COR 2b, LOE B-R. COR 2b, LOE C-LD. COR 1, LOE B-NR.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. The fact that this is syncope makes give it a far lower pretest probability than chest pain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS.
His daughter immediately started CPR and another family member called EMS. The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Initial hsTnI was 384 ng/L.
ECMO Flow was achieved after approximately 1 hour of high quality CPR. Angiography showed normal coronaries. MINOCA: Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease). Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus."
There was no bystander CPR. For this reason we did not believe this was an acute coronary event and did not activate the cath lab. Here is the troponin profile overnight: This is consistent with cardiac arrest without acute coronary occlusion. So a dual chamber pacer is placed with one lead through the coronary sinus to the LV.
There are two types of CPR devices: 1. Load-distributing band CPR devices (LDB) Provide circumferential thoracic compression 2. Piston-driven CPR device (PD) Provide sternal compressions In preclinical settings, CPR devices improve coronary perfusion, cardiac output, ROSC. What’s the evidence so far?
STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial. Based on this, the authors did a literature review and found that there is an increasing rate of ICH and major non-intracranial bleeding starting at ≈60 years of age.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. 3-vessel disease can make resuscitation very difficult, since CPR does not perfuse diseased vessels as well as one would like. He reports feeling nauseated with emesis.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAFB) on the admission ECG.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion.
It is reasonable to administer vasodilators (eg, nitrates, phentolamine, calcium channel blockers) for patients with cocaine-induced coronary vasospasm or hypertensive emergencies. Vasodilators, such as phentolamine and/or nitrates, are reasonable for coronary vasospasm from sympathomimetic poisoning. COR 2a, LOE C-LD. COR 1, LOE C-EO.
Clinical Question : In patients who suffer an OHCA without ST-segment elevation on the post-resuscitation ECG, will early coronary angiogram (CAG) vs. delayed CAG improve outcomes? Emergency vs Delayed Coronary Angiogram in Survivors of Out-of-Hospital Cardiac Arrest: Results of the Randomized, Multicentric EMERGE Trial. Janssens, G.
He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. He underwent coronary stenting (uncertain which artery). See explanation below. The patient went home and, in front of his wife, he collapsed. I do not have the post-resuscitation ECG.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Updates on the Electrocardiogram in Acute Coronary Syndromes. Electrocardiogram patterns in acute left main coronary artery occlusion. References : 1. Nikus KC, Eskola MJ.
What They Did: Single-center, pilot prospective observational cohort trial in Turkey Thrombolysis 25mg of alteplase without a bolus was administered over 6 hours by peripheral IV infusion If hemodynamic instability persisted despite first dose of thrombolysis, a second 6hr infusion of 25mg alteplase without bolus was administered (No patients in the (..)
The assay at my institution, for example, is frequently negative until 4-6 hours after acute coronary occlusion. This rhythm reportedly produced no palpable pulse, and CPR was continued. 30 seconds later, however, the patient began spontaneously moving and CPR was discontinued.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. A middle-age woman with h/o hypertension was found down by her husband.
He underwent CPR and then was shocked out of VF. At times — the initial subtle findings simply represent a phase of "pseudo-normalization" that may occur soon after spontaneous reopening of an acutely occluded coronary artery. Today's patient is high-risk ( ie, in a high "prevalence" group for having an acute coronary event ).
However, vertical flow can result in myocardial injury secondary to coronary artery spasm. Prolonged CPR should be considered as outcomes are generally good, even if asystole is the presenting rhythm. Household supply in the UK and Australia is typically capped at 230v, so children get low-voltage injuries.
Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAFB) on the admission ECG. 30 minutes later, this ECG was recorded: There is less high lateral ST elevation And another 3.5
Data that do not establish neurological risk stratification in the first 6 hours after CA include the patient’s age, duration of CPR, seizure activity, serum lactate level or pH, Glasgow motor subscore in patients who received NMB or sedation, pupillary function in patients who received atropine, and optic nerve sheath diameter (95.3%, 20/21).
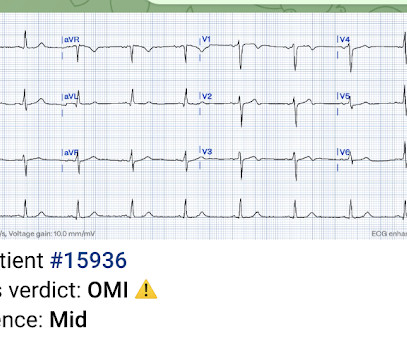
CPR was initiated immediately. As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow).
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. There was no significant difference in cooling method between original cohorts.
CPR was initiated and she subsequently entered into V-Fib storm. For example, a coronary plaque ruptures: the vessel can undergo occlusion, spontaneous reperfusion, maybe reocclusion, again reperfusion, etc. Another ECG is obtained: She suddenly occluded her LAD with a very large territory of viable myocardium at risk!
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. This ALONE is very strong evidence of acute coronary occlusion. Any indications for cath lab activation?
He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. And so it is wise to look at the coronary arteries. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable.
In total, he received approximately 40 minutes of CPR and 7 defibrillation attempts. Coronary spasm causing massive current of injury with shark fin ECG. I would not expect ST-E to vanish in four beats with dissolving thrombus (also we know that the coronaries were clean). I suspect LAD or LM.
CPR was started immediately. Angiogram --Minimal coronary atherosclerosis --No obstructive epicardial coronary artery disease or evidence of plaque rupture noted to explain prolonged QT or ventricular fibrillation cardiacarrest, suspect nonischemic mechanism Echo The estimated left ventricular ejection fraction is 45 %.
Liberal O2 (PaO2 13 to 14kPa (98 to 105mmHg) Initial FiO2 set at 0.6 Liberal O2: 33.9% HR 0.95; 95% CI 0.75 to 1.21; p = 0.69 Results were consistent in all prespecified subgroups Death at 90d Restrictive O2: 28.7% Liberal O2: 31.1% HR 0.93; 95% CI 0.72 Higher MAP: 34.0% HR 1.08; 95% CI 0.84 to 1.37; p = 0.56
Patients who received CPR or experienced reinfarction or very small infarcts due to thrombolysis also displayed Type II T-wave evolution. Global Utilization of Streptokinase and t-PA for Occluded Coronary Arteries. Specificity of Type II for PIRP was 77%. GUSTO-I Investigators. JAMA 1998; 279:387-381. Methods: Hathaway et al.
We could not resuscitate her, but we did have excellent perfusion with LUCAS CPR, such that pulse oximetry had excellent waveform and 100% saturations, end tidal CO2 was 35, and cerebral perfusion monitoring was near normal throughout the attempted resuscitation. Armstrong, MD Arch Intern Med. 1987;147(3):465-469. doi:10.1001/archinte.1987.00370030069014.
Reviewed by: Vicki Currie Article 5: Does occluding the femoral artery during neonatal CPR increase the likelihood of ROSC? (In The goal of chest compressions during neonatal resuscitation is to increase cerebral and coronary blood flow with the intention to achieve a return of spontaneous circulation (ROSC).
The arterial pressure waveform is transduced using the coronary catheter. Normally, the diameter of the coronary artery ostium is much greater than the diameter of the catheter so that catheter engagement does not significantly impair antegrade coronary perfusion. Here is the ECG and arterial waveform during RCA angiography.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content