This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation.
They started CPR. The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion!
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think? No Chest Pain, but somnolent.
There was no bystander CPR. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines.
This post will focus on the key parts of the guideline that affect ED evaluation and management. For patients with OHCA, use of steroids during CPR is of uncertain benefit. Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association 2023 Guideline Updates for 2023 were just published.
ECMO Flow was achieved after approximately 1 hour of high quality CPR. Angiography showed normal coronaries. MINOCA: Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease). Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus."
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. 3-vessel disease can make resuscitation very difficult, since CPR does not perfuse diseased vessels as well as one would like. He reports feeling nauseated with emesis.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion.
This post will focus on the key parts of the guideline that affect ED evaluation and management. It is reasonable to administer vasodilators (eg, nitrates, phentolamine, calcium channel blockers) for patients with cocaine-induced coronary vasospasm or hypertensive emergencies. Top 10 Take Home Pearls 1. COR 2a, LOE C-LD.
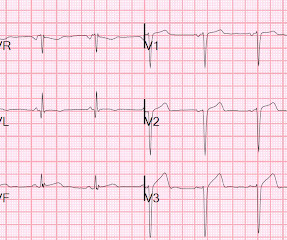
Here is his ECG on presentation to the ED, approximately 45 minutes after onset of pain, but with pain improving since onset: What is your interpretation? The initial ECG was interpreted as "normal" by the computer ( Algorithm: Marquette GE / 12SL ) and "no acute ischemic changes" by the ED physician.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Updates on the Electrocardiogram in Acute Coronary Syndromes. at the time of the ECG.
About an hour later, he was then found on the floor in cardiac arrest in the ED. He underwent CPR and then was shocked out of VF. The history in today's case — was that of a man in his 70s who presented to the ED for 2 hours of chest pain , that was still present on arrival in the ED. But we should not be surprised.
However, vertical flow can result in myocardial injury secondary to coronary artery spasm. Prolonged CPR should be considered as outcomes are generally good, even if asystole is the presenting rhythm. In: Walls RM, ed. Household supply in the UK and Australia is typically capped at 230v, so children get low-voltage injuries.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
The patient arrived in the ED and had this ECG recorded: Interpretation? Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAFB) on the admission ECG.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chest pain associated with shortness of breath for the last 2 days. CPR was initiated and she subsequently entered into V-Fib storm. If this patient was discharged from the ED she very likely would have died. Thanks, Sam! Normal ECG.”
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Vitals were HR 58 BP 167/70 R20 sat 96%.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
CPR was started immediately. I was texted this ECG in real time, but it turns out to actually be the 2nd one recorded in the ED. ECG #4 — This is the 3rd ECG that was done in this case ( obtained ~1 hour after arrival in the ED ). A 60-something woman presented after a witnessed cardiac arrest. She was never defibrillated.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. And so it is wise to look at the coronary arteries. He was moderately hypoxic.
Her prehospital ECG was identical to her first ED ECG, and the cath lab was activated: There is massive ST elevation (greater than 15 mm) in V2 and V3, with ST elevation in I and aVL and reciprocal ST depression in II, III, aVF. Peterson ED, Hathaway WR, Zabel KM, et al. Hathaway WR, Peterson ED, Wagner GS, et al.
Here is his ED ECG: There is obvious infero-posterior STEMI. We could not resuscitate her, but we did have excellent perfusion with LUCAS CPR, such that pulse oximetry had excellent waveform and 100% saturations, end tidal CO2 was 35, and cerebral perfusion monitoring was near normal throughout the attempted resuscitation.
Sex ed” sucks. They believe that Sex Ed programs are irrelevant to real-life experience and contain inadequate discussion of important issues, including consent or positive sexual relationships. Reviewed by: Vicki Currie Article 5: Does occluding the femoral artery during neonatal CPR increase the likelihood of ROSC? (In
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content