This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. They started CPR.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
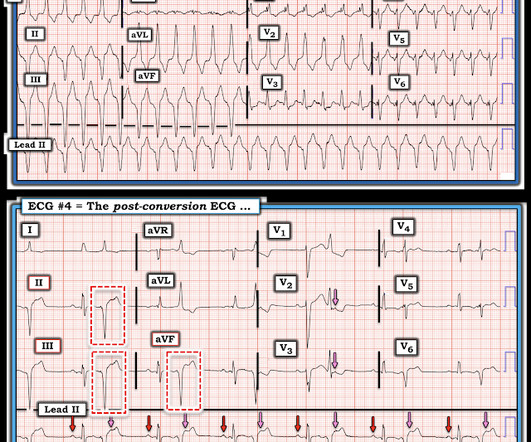
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. The 3rd inferior lead ( = lead II ) — shows definite ST-T wave flattening.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. There is no definite evidence of acute ischemia. (ie,
When I saw the ECG of this patient I saw that there was definitely something "off". She spontaneously converted (Defibrillation was not performed). Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. A repeat magnesium level was not drawn prior to coronary angiography.
Today's case reminds us of the intuitive logic that if a patient has a shockable arrest ( ie, VFib ) — and following successful defibrillation shows evidence of acute OMI ( even if STEMI criteria are not necessarily fulfilled ) — that such patients have much to gain from immediate cath with PCI. ( The April 8, 2022 post by Drs.
They are not premature, by definition. We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. The green arrows, however, do show premature complexes. potassium) were within normal parameter.
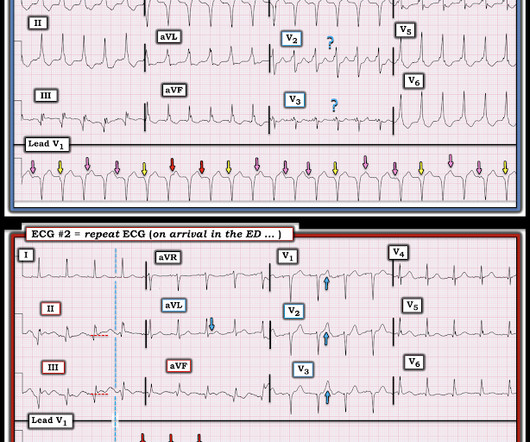
There is definite change in the morphology of the waveforms and there is also significant change in the polarity of the QRS complexes in the precordial leads. After amiodarone and several defibrillations and about 20 minutes after initial arrest, stable ROSC was achieved. Other coronaries were normal. Is there OMI?
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. It was stented.
She was defibrillated and resuscitated. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. One need not have obstructive coronary disease to have occlusive thrombus!
She was never seen to be in ventricular fibrillation and was never defibrillated. Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. BP gradually rose.
Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Transient ST-segment myocardial infarction: a new category of high risk acute coronary syndrome?
She was never defibrillated. Angiogram --Minimal coronary atherosclerosis --No obstructive epicardial coronary artery disease or evidence of plaque rupture noted to explain prolonged QT or ventricular fibrillation cardiacarrest, suspect nonischemic mechanism Echo The estimated left ventricular ejection fraction is 45 %.
Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc. He was defibrillated immediately and had return of normal mental status.
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
Fortunately , you don't need to make a definite diagnosis. Second , when you have a rhythm problem, you are likely to be able to fix the problem with electricity (cardioversion, defibrillation, pacing). Fifth , potential management actions are in your hands; you do not need to request a coronary interventionalist or cath lab team.
The submitter started the patient on amiodarone and arranged implantation of a defibrillator. == MY Comment , by K EN G RAUER, MD ( 12/27 /2024 ): == Superb discussion by Dr. Frick in today's case, that highlights a series of important points regarding the ECG recognition of stable VT ( V entricular T achycardia ).
ONLY give opiates if the pain is intolerable or you will activate the cath lab at the first objective evidence of coronary ischemia. In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). The patient was taken to lab for coronary angiography.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content