This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. The proof of this is that only 5% of patients enrolled had acute coronary occlusion.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The patient was brought to the ED and had this ECG recorded: What do you think? The patient was brought to the ED and had this ECG recorded: What do you think? It also does not uniformly indicate severe coronary disease.
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Here is the initial ED ECG. What do you think?
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. It is unknown when this pain recurred and became constant.
This post will focus on the key parts of the guideline that affect ED evaluation and management. With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed. COR 2b, LOE C-LD. COR 3, No benefit, LOE B-R. COR 2b, LOE B-R.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Despite immediate chest compressions, and multiple rounds of defibrillation, he could not be resuscitated. Breath sounds were clear in all lung fields.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. Ventricular fibrillation is not only caused by acute coronary syndrome.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The arrhythmia spontaneously converted before defibrillation was achieved. This is an ominous sign.
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). There is a relatively normal QRS yet there is STD maximal in V2-V4, which resolves from V4 to V6.
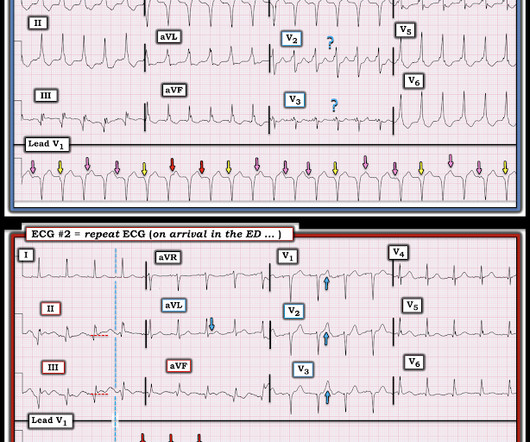
On arrival to the ED, this ECG was recorded: What do you think? Although predicting the "culprit" artery of acute coronary occlusion is often straightforward ( ie, based on the distribution of leads with ST elevation and leads with reciprocal ST depression ) — this is not always the case. This prompted cath lab activation.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Chou’s Electrocardiography in Clinical Practice (6th ed). Question 2: What explains the conduction abnormalities? Surawicz, B.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm.
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
Here is his ECG on presentation to the ED, approximately 45 minutes after onset of pain, but with pain improving since onset: What is your interpretation? The initial ECG was interpreted as "normal" by the computer ( Algorithm: Marquette GE / 12SL ) and "no acute ischemic changes" by the ED physician.
She was defibrillated and resuscitated. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. One need not have obstructive coronary disease to have occlusive thrombus!
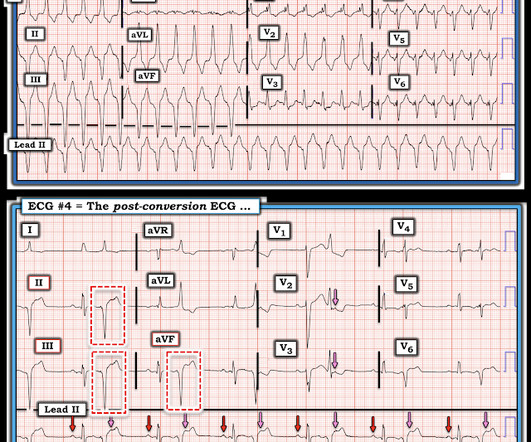
She was never defibrillated. I was texted this ECG in real time, but it turns out to actually be the 2nd one recorded in the ED. ECG #4 — This is the 3rd ECG that was done in this case ( obtained ~1 hour after arrival in the ED ). As was seen in this case — defibrillation and/or overdrive pacing may be needed.
If the patient only had these two ECGs recorded, it would have missed the transient time between them which were STEMI positive, and the patient would then have arrived at the ED as “serial ECGs STEMI negative." Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Meyers et al.
When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. 90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. CPR was initiated immediately.
Here is his ED ECG: There is obvious infero-posterior STEMI. At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. Medics stated that he had not been taking his clopidogrel for 2 weeks. He appeared to be in shock.
We talk about the nitty-gritty details of a well-run cardiac arrest, with Scott Weingart of Emcrit (@emcrit), ED intensivist. Takeaway lessons Resources We talk about the nitty-gritty details of a well-run cardiac arrest, with Scott Weingart of Emcrit ( @emcrit ), ED intensivist. Learn more at the Intensive Care Academy!
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
Second , when you have a rhythm problem, you are likely to be able to fix the problem with electricity (cardioversion, defibrillation, pacing). Fifth , potential management actions are in your hands; you do not need to request a coronary interventionalist or cath lab team. Again the clinical history is helpful.
The submitter started the patient on amiodarone and arranged implantation of a defibrillator. == MY Comment , by K EN G RAUER, MD ( 12/27 /2024 ): == Superb discussion by Dr. Frick in today's case, that highlights a series of important points regarding the ECG recognition of stable VT ( V entricular T achycardia ).
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. She was brought to the ED in a deep coma with GCS of 3, with vital signs, and an ECG was recorded: What do you think? Moreover, it does not follow a coronary distribution very well.
She underwent coronary angiography which showed thrombotic occlusion of an RPL branch s/p aspiration thrombectomy. Throughout this process, the patient had repeated VF and was defibrillated 8 times. Written by Willy Frick A young woman with a history of paroxysmal nocturnal hemoglobinuria presented with acute substernal chest pain.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). CT coronary angiogram showed a hypoplastic RCA and dominant LCx. The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. No PVCs are seen. There were no plaques or stenoses.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content