This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR. Cardiology agreed. Initial trop ~200.
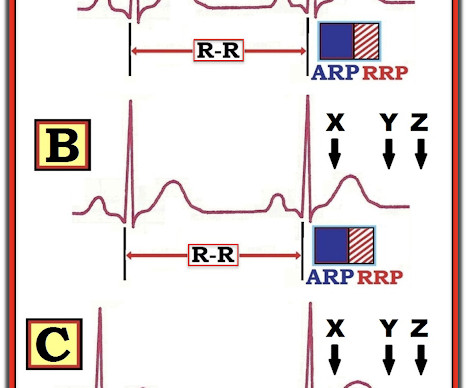
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Beats 9-12 : Continuation of the previously described events, all inducible by the pause (and thus, prolongation of refractoriness) created by the PVC of Beat 8. Question 2: What explains the conduction abnormalities?
After resuscitation and defibrillation , there were no more episodes of TdP. A coronary angiogram was done that did not show significant coronary artery disease. A coronary angiogram was done that did not show significant coronary artery disease. Below is the patient’s 12 lead ECG following defibrillation.
She was defibrillated and resuscitated. Takotsubo is a sudden event, not one with crescendo angina. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronary artery disease, but there was spontaneous coronary artery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
Back to the case: After the patient was roomed, he revealed that he had undergone several episodes of syncope in the last 24 hours with each event resulting in a shock during which his wife reported that he would immediately awaken. The most recent event had occurred just before being triaged.
Side note: contemporary troponin drawn 1 hour after acute LAD occlusion should usually be negative, unless the event has been going on longer than the patients symptoms. The assay at my institution, for example, is frequently negative until 4-6 hours after acute coronary occlusion. It should have been shocked at least 10 seconds ago.
12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC. In total, he received approximately 40 minutes of CPR and 7 defibrillation attempts. Coronary spasm causing massive current of injury with shark fin ECG.
Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Transient ST-segment myocardial infarction: a new category of high risk acute coronary syndrome?
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. This study failed to do so. 5% vs. 58%!! As per Dr.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. It is unknown when this pain recurred and became constant.
Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc. He was defibrillated immediately and had return of normal mental status.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e
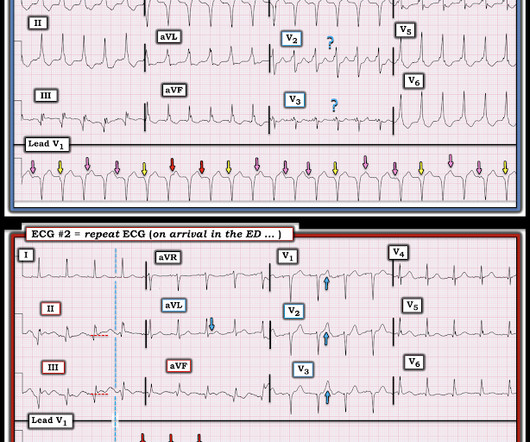
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The most common way is by delivering a lead into the coronary sinus ostium in the RA, which wraps around the posterolateral portion of the LV. ECG 1 What do you think?
The submitter started the patient on amiodarone and arranged implantation of a defibrillator. == MY Comment , by K EN G RAUER, MD ( 12/27 /2024 ): == Superb discussion by Dr. Frick in today's case, that highlights a series of important points regarding the ECG recognition of stable VT ( V entricular T achycardia ).
ONLY give opiates if the pain is intolerable or you will activate the cath lab at the first objective evidence of coronary ischemia. In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). The patient was taken to lab for coronary angiography.
She underwent coronary angiography which showed thrombotic occlusion of an RPL branch s/p aspiration thrombectomy. Throughout this process, the patient had repeated VF and was defibrillated 8 times. This patient had been seen 5 days earlier at another hospital where she underwent aspiration thrombectomy for an acute event.
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. Moreover, it does not follow a coronary distribution very well. The coronaries were clean. Mistaking such cases as an acute cardiac event is not uncommon because of these ECG changes.
The arterial pressure waveform is transduced using the coronary catheter. Normally, the diameter of the coronary artery ostium is much greater than the diameter of the catheter so that catheter engagement does not significantly impair antegrade coronary perfusion. She was defibrillated perhaps 25 times.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content