This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. This study failed to do so. 5% vs. 58%!!
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. They started CPR.
Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients. Many of these OHCAs are due to ventricular fibrillation or pulseless VT.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Breath sounds were clear in all lung fields.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. So it can miss some OMI.
Emergent coronary angiography is not recommended over a delayed or selective strategy in patients with ROSC after cardiac arrest in the absence of ST-segment elevation, shock, electrical instability, signs of significant myocardial damage, and ongoing ischemia (Level 3: no benefit). COR 2b, LOE C-LD. COR 3, No benefit, LOE B-R.
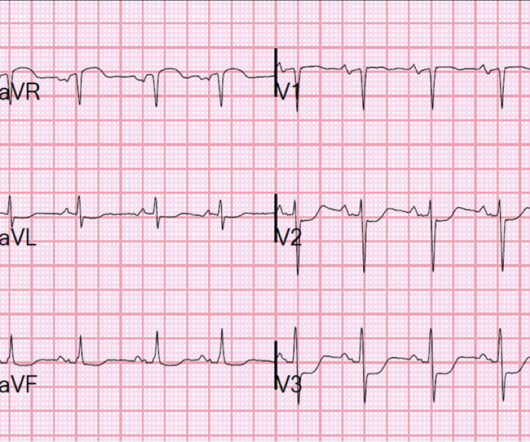
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
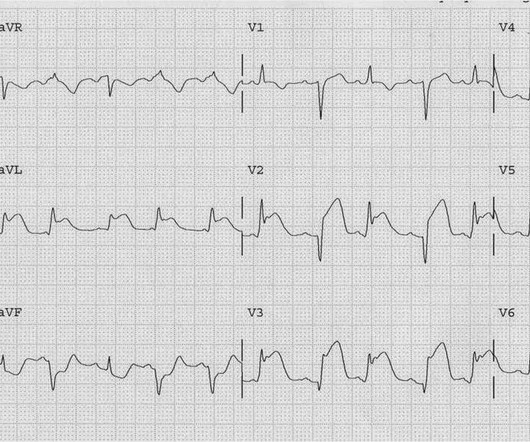
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Smith Comment: Is is common for the artery to be open at angiogram in OMI, including full STEMI.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. Ventricular fibrillation is not only caused by acute coronary syndrome. We found that 38% of out of hospital ventricular fibrillation was due to STEMI.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). He required multiple defibrillations within a period of a few hours. The below ECG was recorded. He was taken immediately to the cath lab.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Instead we discussed 5 minute delays for the STEMI(+) OMI patients.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e STEMI , ST-segment elevation acute myocardial infarction ). STEMI , ST-segment elevation acute myocardial infarction ). due to reciprocal ST-segment depressions in V1, V2, V3).
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. The next day, and angiogram showed normal coronary arteries. Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI. His initial ECG is shown here.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. There is atrial fibrillation.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronary artery disease, but there was spontaneous coronary artery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
She was never seen to be in ventricular fibrillation and was never defibrillated. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. BP gradually rose. Kurkciyan et al.
There are a few subtle signs of coronary occlusion here. He was defibrillated. Anterolateral STEMI. He had an ECG recorded: Sinus Rhythm. This was read as normal by the emergency physician and by the computer. QTc is 400 ms. What do you think? First , look at V4-V6. The T-wave is almost as tall as the R-wave. This should not be.
She was defibrillated and resuscitated. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. One need not have obstructive coronary disease to have occlusive thrombus!
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc.
The assay at my institution, for example, is frequently negative until 4-6 hours after acute coronary occlusion. After the second defibrillation the patient had an organized rhythm: Bradycardic escape/agonal rhythm, with large ST deviations. A repeat ECG was done: Obvious anterolateral wall STEMI.
When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. 90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX.
It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately.
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. Moreover, it does not follow a coronary distribution very well. From this site.
The arterial pressure waveform is transduced using the coronary catheter. Normally, the diameter of the coronary artery ostium is much greater than the diameter of the catheter so that catheter engagement does not significantly impair antegrade coronary perfusion. She was defibrillated perhaps 25 times.
She underwent coronary angiography which showed thrombotic occlusion of an RPL branch s/p aspiration thrombectomy. Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content