This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. This was deemed “non-specific” by the ED physicians. Type I ischemia.
The acute coronary syndrome work-up is negative but she is Well’s high and needs a CTPA to rule-out a pulmonary embolism. Part of the difficulty with this topic is the inconsistent definition of contrast-induced nephropathy. A common definition is an increase in creatinine level by 25% or an absolute increase of 0.3
The ECG does not show any definite signs of ischemia. Why Was Cardiac Cath Negative for Coronary Disease? Use ß-blockers with caution ( as they may aggravate coronary spasm ). Given the potential triggering effect of smoking on coronary spasm — absolute abstinence from smoking is essential! The below ECG was recorded.
Differentiating between the two is difficult as multiple proposed diagnostic criteria have yet to demonstrate sufficient sensitivity or specificity for a definitive diagnosis. Risk factors that increase the likelihood of VT include history of previous myocardial infarction, known coronary artery disease, and structural heart disease.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. And what do you want to do?
Past medical history includes coronary stenting 17 years prior. Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. Definitive diagnosis that ECG #1 is in fact VT is more than academic.
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. This included the addition several new STEMI equivalents [4] on ECG that warrant “prompt evaluation for emergency coronary angiography.”
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. In an attempt to clarify language, a consensus definition was developed. per 100,000 to 11 per 100,000 [Rosso].
Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. A false positive cath lab activation is also off course acceptable for this diagnosis if you cannot get an emergent coronary CT angiogram. Each main coronary artery (LAD, RCA and LCx) are shown in separate images.
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI. It is unknown when this pain recurred and became constant.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
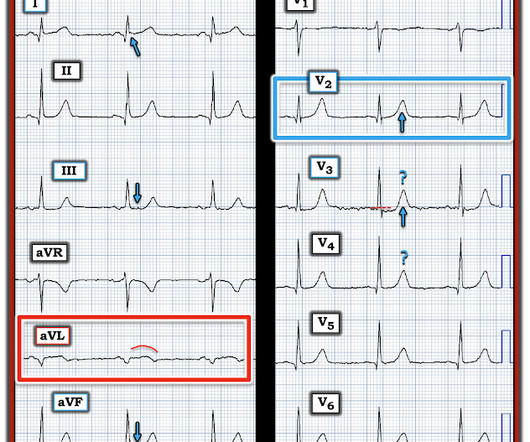
What lowered my confidence in calling ECG #1 a definite OMI — was the finding of somewhat similar-appearing , upright T waves with slight-but-real J-point ST elevation in so many leads ( ie, leads I,II,aVF; V2-thru-V6 ). Once I identified leads V4 and V5 as definitely abnormal — I looked closer at neighboring leads.
Thus, this does NOT meet STEMI criteria (though, as of 2022, it is a formal "STEMI equivalent", assuming everyone agrees that this is de Winter morphology, for which there is currently no objective definition). Even if a patient's ECG does meet STEMI criteria, it may not be perceived so. What a farce.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. 1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. Attached is the first ECG. Isn’t VT ALWAYS “wide”?
When I saw the ECG of this patient I saw that there was definitely something "off". The patient was referred for coronary angiography which did not reveal any atherosclerotic changes. A formal echo at the PCI center after coronary angiography revealed a large septal and apical WMA. Troponin I peaked at 769 ng/L.
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Although predicting the "culprit" artery of acute coronary occlusion is often straightforward ( ie, based on the distribution of leads with ST elevation and leads with reciprocal ST depression ) — this is not always the case. See Discussion in the June 29, 2024 post of Dr. Smith' ECG Blog ). The April 8, 2022 post by Drs.
Therefore, this does not meet the definition of myocardial infarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. You can see the deficiency of the definition of MI. Two negative troponins do not exclude the possibility of short-lived acute coronary occlusion.
Thus, there are some suspicious abnormalities, but no definite signs of ischemia. But the definition misses the point. It is a coronary occlusion with a substantial myocardial territory at risk, that showed only very subtle ST changes. There are thin and normal inferior Q-waves. It is very subtle but real.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech. No ECG was ordered on Day #1.
Upon further research in the 1970’s, retrospective data from autopsies of those patients showed coronary aneurysms 5 Pathophysiology: Kawasaki Disease is a vasculitis of medium sized arteries. Tomisaku Kawasaki, who noticed 50+ similar pediatric presentations between the years 1961 and 1967.
Finally — there is the clinical reality that a patient who has a "baseline" ECG that manifests a repolarization variant — may at some point develop acute coronary occlusion that in part is masked by benign-appearing ECG characteristics of the underlying repolarization variant. It is clearly missed by the conventional algorithm.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. All coronary arteries were patent without atherosclerotic change. Only after troponin returned elevated was an Echo was done, revealing a definite wall motion abnormality.
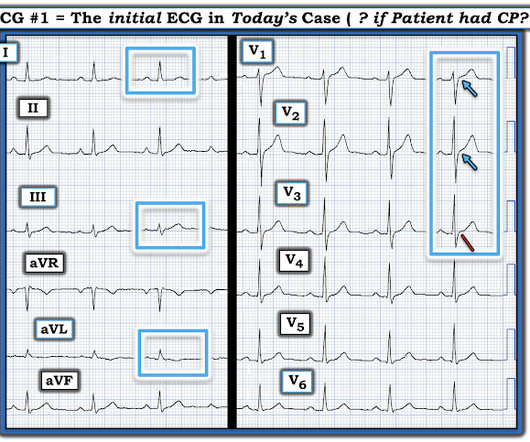
However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). Is this: 1. Figure-1: I have labeled the initial ECG in today's case. (
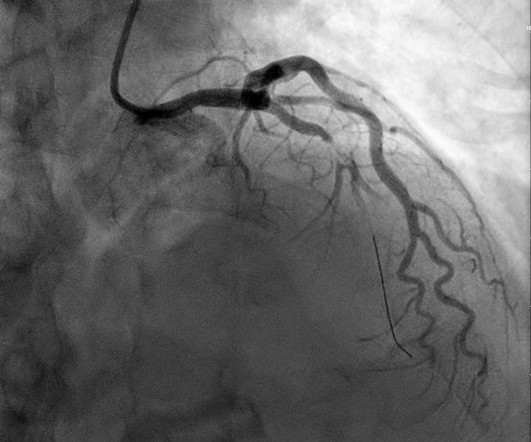
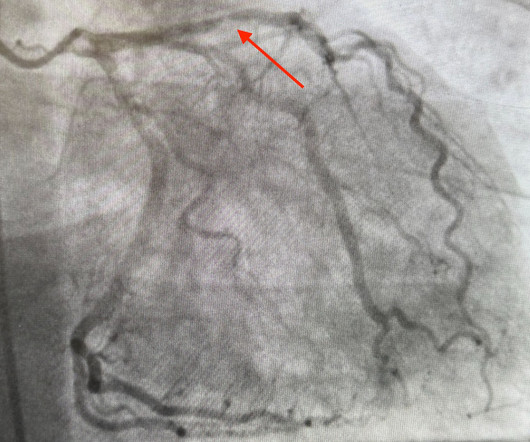
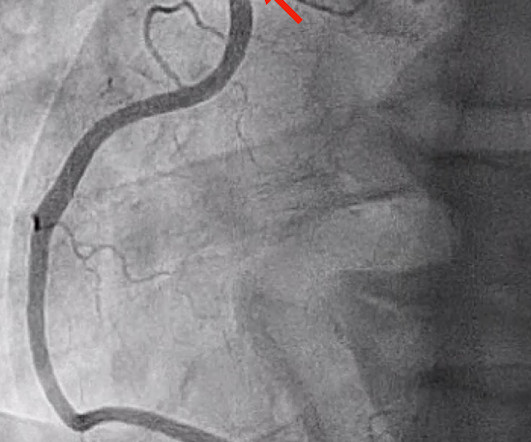
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. There is no definite evidence of acute ischemia. (ie,
Angiogram: Severe two-vessel coronary artery disease with possible co-culprits (90% proximal circumflex, 70% mid/distal RCA) in the setting of non-ST elevation myocardial infarction. Marked ST depression from multi-vessel coronary disease serves to attentuate what would have been ST elevation in leads II and aVF ).
Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) have perfect coronary flow by the time of angiogram. Serial tracings often show “ dynamic ” ST-T wave changes — which in a patient with CP, allow prompt definitive diagnosis that might not have been obvious with just a single tracing.
They are not premature, by definition. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g.
See the variety of Left Main Occlusion ECGs here: How does Acute Total Left Main Coronary occlusion present on the ECG? == MY Comment , by K EN G RAUER, MD ( 5/3 /2024 ): == Most patients with acute LMain Occlusion do not survive to make it to the hospital. Left Main Non-Occlusive ACS presents with widespread ST Depression and STE in aVR.
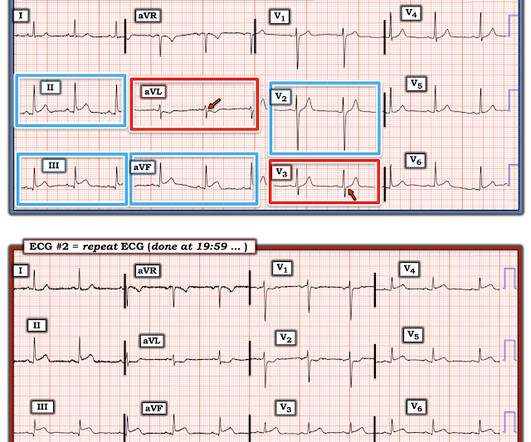
Serial ECGs enhance the diagnosis of acute coronary syndrome. Although recognition of OMI was not affected by administration of morphine in this case, use caution with analgesia in ongoing ACS without a definitive plan for angiography. Although tiny in size — the BLUE arrows highlight definite ST elevation in leads I and aVL.
As per Dr. McLaren — today's patient was lucky in that the acute coronary occlusion spontaneously reperfused — and the patient remained pain-free. The Need for Immediate Transport? Limb lead findings in ECG #2 look more hyperacute than they did in ECG #1 — because of subtle-but-real increased ST segment straightening in leads I, III and aVL.
There is maybe no definite answer and arguments can be made for the different scenarios. An MRi was not done for this patient and a definite answer maybe cannot be obtained. with the important message that sometimes ( especially in retrospect! ) — a definite diagnosis can not be made. There is reconstitution of R waves V3-V6.
The coronary angiography showed a 100% ostial main (obtuse) marginal occlusion!" Dominant right coronary, atherosclerotic and calcified. Presence of a single coronary lesion: occlusion of the ostial main marginal. ECG #1 — shows such subtle but-definitely-present changes in multiple leads: The rhythm is sinus at 80-85/minute.
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). Answer: This is MINOCA -- Myocardial Infarction with Non-Obstructive Coronary Arteries. His troponin peaked at 10.310 ng/mL and trended down. The name is self-explanatory.
Extracorporeal membrane oxygenation Of patients with out-of-hospital cardiac arrest presenting to the ED in refractory VF, a majority have significant coronary artery disease, much of which is amenable to percutaneous coronary intervention. Circulation. 2019;139(12):e530-e552. Yannopoulos D, et al. J Am Coll Cardiol.
Yet despite this remarkable flaw in the STEMI-paradigm — a substantial number ( if not a frank majority ) of clinicians continue to apply outdated criteria when interpreting ECGs, by refusing to consider prompt cath for definitive diagnosis and reperfusion therapy just because a millimeter-based definition for acute STEMI is not satisfied.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. that is, show a pattern of labile ST-T wave changes not due to an acute coronary event. I personally can hardly wait for that future version! Some patients do this.
I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. So this study is worthless and must be ignored.
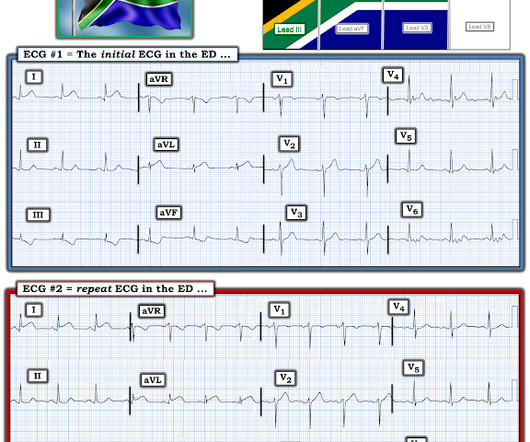
The initial ECG in today's case was recognized as definitely abnormal — but the question arose as to whether this ECG indicated old infarction vs a new acute event. The "good news" — is that a cardiac-related cause of syncope is unlikely if the initial ECG is normal, and cardiac monitoring in the ED fails to reveal significant arrhythmia.
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. Additionally, no current high-quality literature exists regarding the definitive indications for REBOA placement.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content