This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
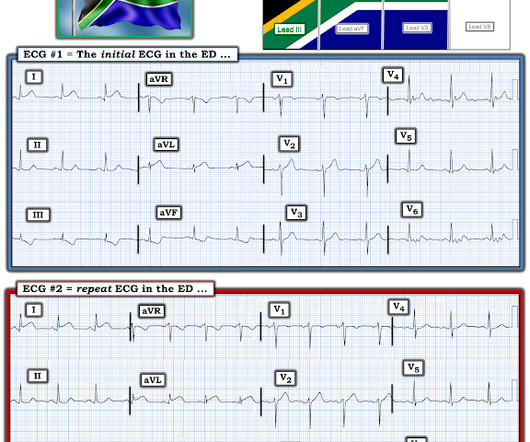
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians. Thus, the ED admission ECG changes cannot be blamed on LVH. The fall was not a mechanical etiology.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
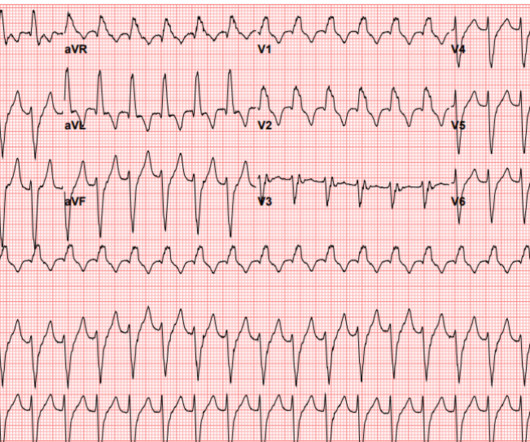
The Case A 41-year-old male presents to the ED with constant palpitations for one day. Differentiating between the two is difficult as multiple proposed diagnostic criteria have yet to demonstrate sufficient sensitivity or specificity for a definitive diagnosis. Discussion Fascicular VT is a distinct subgroup of idiopathic VT.
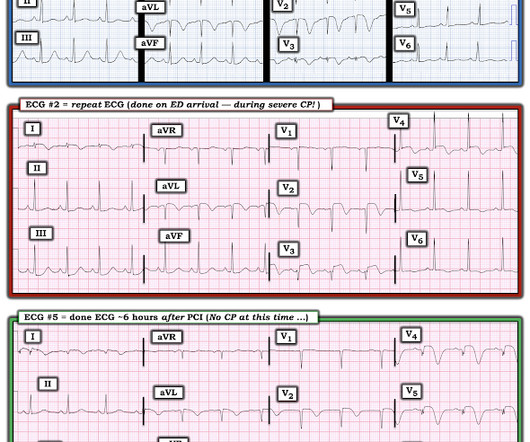
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. It’s judicious, then, to arrange for coronary angiogram.
The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! sodium bicarbonate.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion.
Past medical history includes coronary stenting 17 years prior. Initial ED ECG: What do you think? Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
More past history: hypertension, tobacco use, coronary artery disease with two vessel PCI to the right coronary artery and circumflex artery several years prior. Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI. It is unknown when this pain recurred and became constant.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. 1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. Attached is the first ECG. Isn’t VT ALWAYS “wide”?
Here is his initial ED ECG: What do you think? Then the ED doc would be dependent on that first ECG. It must have re-occluded between the ED and the cath lab) --Lesion was stented. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) have perfect coronary flow by the time of angiogram.
A 3-year-old male with no past medical history presents to the ED with one week of daily fevers >102°F associated with four days of rash on the trunk. We’ll keep it short, while you keep that EM brain sharp. Tomisaku Kawasaki, who noticed 50+ similar pediatric presentations between the years 1961 and 1967. C) for the past week.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
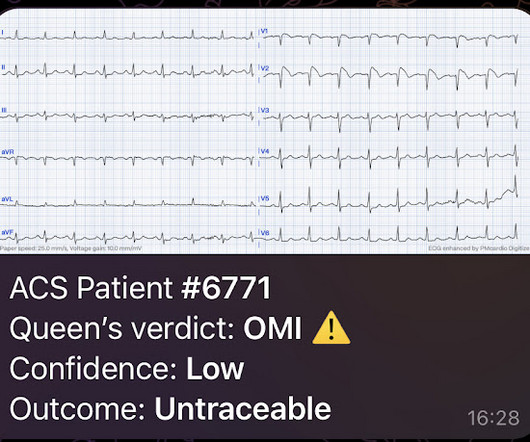
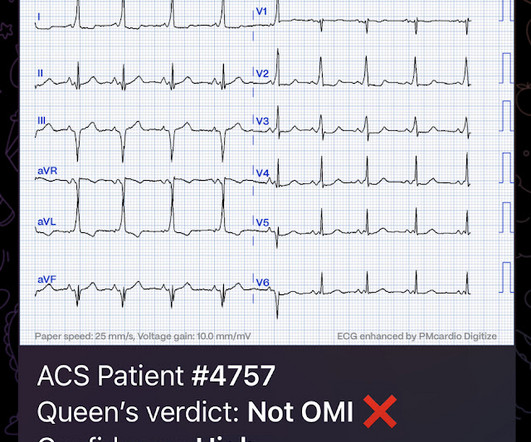
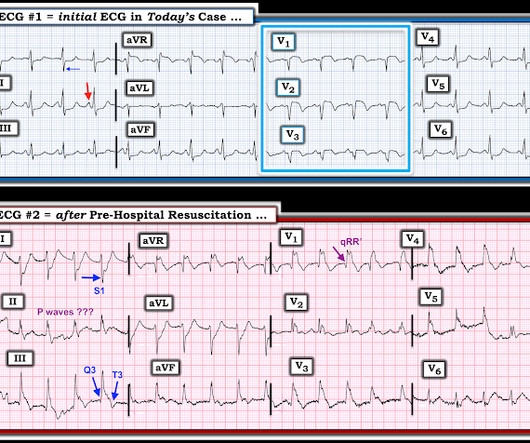
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. Figure-1: I've labeled the initial EMS ECG and the 1st 12-lead tracing done on arrival in the ED.
However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). Is this: 1. Figure-1: I have labeled the initial ECG in today's case. (
On arrival to the ED, this ECG was recorded: What do you think? Although predicting the "culprit" artery of acute coronary occlusion is often straightforward ( ie, based on the distribution of leads with ST elevation and leads with reciprocal ST depression ) — this is not always the case. This prompted cath lab activation.
They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2]
When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think? The initial ECG in today's case was recognized as definitely abnormal — but the question arose as to whether this ECG indicated old infarction vs a new acute event.
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. Coronary artery disease in patients with out-of-hospital refractory ventricular fibrillation cardiac arrest. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S. Circulation. 2019;139(12):e530-e552.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. This is another case sent by the undergraduate (who is applying to med school) who works as an EKG tech. No ECG was ordered on Day #1.
Finally — there is the clinical reality that a patient who has a "baseline" ECG that manifests a repolarization variant — may at some point develop acute coronary occlusion that in part is masked by benign-appearing ECG characteristics of the underlying repolarization variant. It is clearly missed by the conventional algorithm.
He presented to the ED after 30 minutes, now also feeling weak. Thus, there are some suspicious abnormalities, but no definite signs of ischemia. But the definition misses the point. It is a coronary occlusion with a substantial myocardial territory at risk, that showed only very subtle ST changes. He was diaphoretic.
They are not premature, by definition. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. Some patients do this.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" On arrival to the ED, while waiting for cath lab team, he obtained another ECG: You can now see the full voltage of the high-voltage QRS, likely with some degree of LVH. Both were awake and alert with normal vital signs.
In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. 4-6] In figures 1-4, specifically during the episodes of NSVT, there is a mostly regular cadence with preserved definition of both QRS and T. Chou’s Electrocardiography in Clinical Practice (6th ed).
Keep in mind the presenting History ( ie, a 50yo presenting to a rural ED with a 1-hour history of CP radiating to the back and jaw — and an initial ECG labeled as "normal" by the computer interpretation ). As you comtemplate the above issues to address — Take another LOOK at these first 2 ECGs in today's case.
As part of her work up in the ED an ECG was recorded. There is maybe no definite answer and arguments can be made for the different scenarios. An MRi was not done for this patient and a definite answer maybe cannot be obtained. The patient is a 60 something female. She was febrile and hypotensive at presentation.
But the paramedic and the ED physician in this case did not subscribe to this idea. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. So this study is worthless and must be ignored.
An ED ECG, if recorded with pain, should show LAD OMI. So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5. The Cath lab was activated.
Imagine you just started your ED shift. Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. R wave V4 9mm) C T of the coronary arteries showed no lesions. That said, this patient did present to the ED with "new CP" — and.
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. A 25-year-old man presents to the ED via EMS after he sustained a gunshot wound to the left flank.
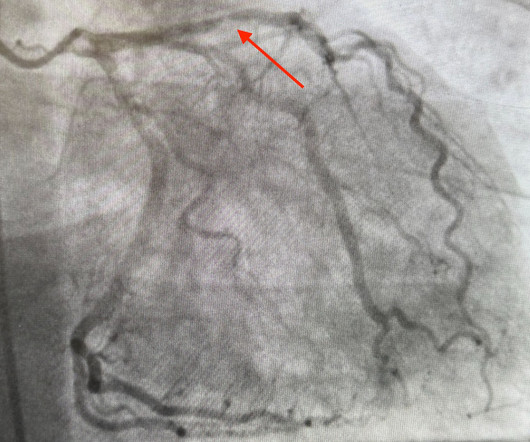
He reported typical chest pain since 4H AM and arrived at our ED at 10h with ongoing chest pain. The coronary angiography showed a 100% ostial main (obtuse) marginal occlusion!" Dominant right coronary, atherosclerotic and calcified. Presence of a single coronary lesion: occlusion of the ostial main marginal.
On arrival in the ED, the patient denied any symptoms at all. No chest pain, no shortness of breath, no back pain, no numbness, weakness, tingling, no seizures or history of seizures, First ED ECG This still shows apparent inferior OMI. The patient was g iven full dose aspirin and the medics activated the Cath Lab.
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Angiography showed normal coronaries. A followup ECG was recorded 2 days later: No definite evidence of infarction. MINOCA: Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease). Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus."
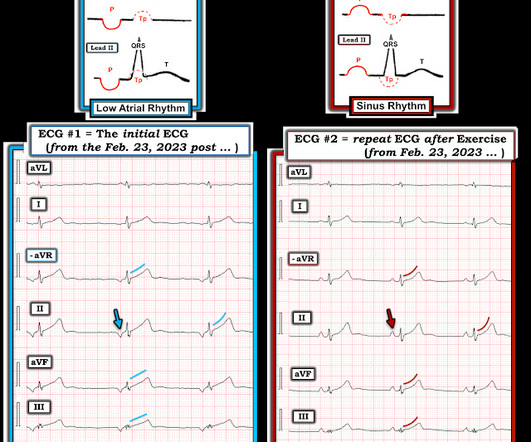
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. The angiogram showed completely normal coronary arteries. Triage ECG: What do you think? Note that the Tp is oppositely directed to the P wave.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
link] A 30 year-old woman was brought to the ED with chest pain. The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This is written by Brooks Walsh.
She went to angio and had normal coronaries. She was briefly resuscitated and made it to the ED alive, long enough to have another ECG: This could be all due to RV strain or the STE in inferor leads could also be due to supply demand mismatch (type II STEMI) She was given 100 mg of tPA but arrested again and could not be resuscitated.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Such cases are classified as MINOCA (Myocardial Infarction with Non-Obstructed Coronary Arteries). It can only be seen by IVUS.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content