This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Differentiating between the two is difficult as multiple proposed diagnostic criteria have yet to demonstrate sufficient sensitivity or specificity for a definitive diagnosis. Risk factors that increase the likelihood of VT include history of previous myocardial infarction, known coronary artery disease, and structural heart disease.
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. In October 2022, the American College of Cardiology released an updated expert consensus decision regarding the evaluation of chest pain in the emergencydepartment.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 2 What do you think?
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. The undergraduate is now willing to identify himself: Hans Helseth. No ECG was ordered on Day #1.
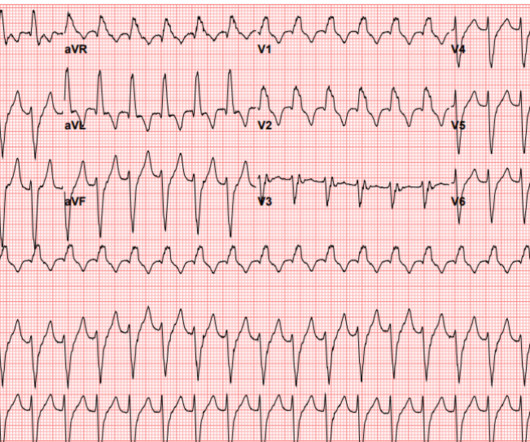
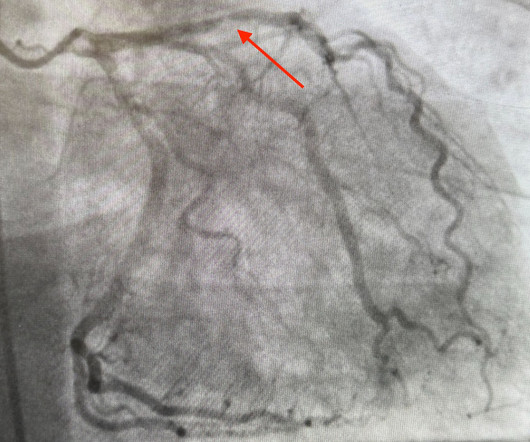
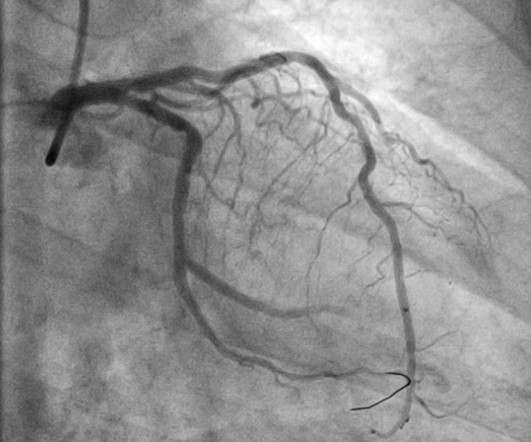
Angiogram: Severe two-vessel coronary artery disease with possible co-culprits (90% proximal circumflex, 70% mid/distal RCA) in the setting of non-ST elevation myocardial infarction. Marked ST depression from multi-vessel coronary disease serves to attentuate what would have been ST elevation in leads II and aVF ).
Many systems now refrain from showing computer "normal" ECGs to the busy emergency physicians at triage because of very poorly conceived articles that say that if the computer algorithm says "normal," the emergency physician should not be bothered. It is clearly missed by the conventional algorithm.
emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. Adult cardiac arrest in the emergencydepartment – A Swedish cohort study. Coronary artery disease in patients with out-of-hospital refractory ventricular fibrillation cardiac arrest. Circulation.
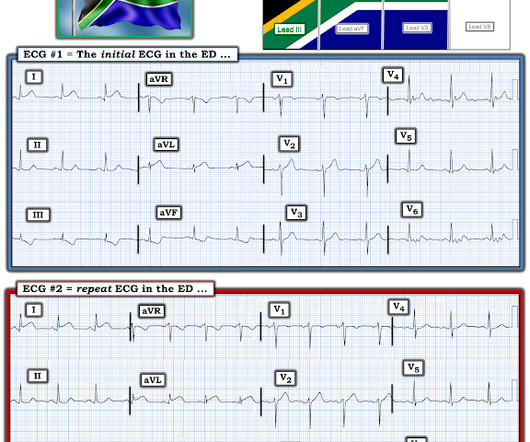
A 50 year old presented to the emergencydepartment of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chest pain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. The Need for Immediate Transport?
She presented to the emergencydepartment after a couple of days of chest discomfort. However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. What is your assessment?
Am J Emerg Med. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. 2022 Jan;51:384-387.
She was unable to be defibrillated but was cannulated and placed on ECMO in our EmergencyDepartment (ECLS - extracorporeal life support). Angiography showed normal coronaries. A followup ECG was recorded 2 days later: No definite evidence of infarction. An elderly woman had sudden ventricular fibrillation.
Open angle Closed angle Definitions Increased resistance to aqueous outflow through the trabecular meshwork. Transient vision loss defined as vision loss <24 hours. Persistent vision loss defined as loss of vision >24 hours. Bagheri 2015 ). Decreased visual acuity, Cup to disc ratio >0.6 Cup to disc ratio >0.6
It was ongoing on arrival in the emergencydepartment. STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. Am J Emerg Med 2023 2. What do you think?
The pain resolved as he arrived to the emergencydepartment. He was definitely pain free by the time of arrival at his ED room. The 4th Universal Definition of MI calls this Cardiac Procedural Myocardial Injury. He had 2 episodes over the past 2 days of similar chest tightness. BP was 200/100. Here was his triage ECG.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Relationship between an in-farct related artery, acute total coronary occlusion, and mortality in patients with ST-segment and non-ST-segment myocardial infarction.
A prospective validation of the HEART score for chest pain patients at the emergencydepartment. External validation of the emergencydepartment assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP). Am J Emerg Med 2020 3. Backus BE, Six AJ, Kelder JC, et al. Int J Cardiol 2013 2. Lancet 2015 6.
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? There is definite STE inferior and lateral but it just doesn't look like true positive STE to me. No baseline was available for comparison.
There is perhaps a tiny J-wave in several of the QRS complexes in V3, but it would not be enough to definitively say there is a J-wave. Lead aVL, for example, has a definite J-wave. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria. Stat echo would also be helpful. mV compared to 0.05-0.1
The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. He had no symptoms of ACS.
Here is a video lecture of subtle LAD occlusion: One hour lecture on Subtle ECG Findings of Coronary Occlusion The 3-variable formula comes from this paper: Smith SW et al. He went for Coronary bypass (CABG). above which one should definitely be worried and get serial ECGs. 4-variable version still to come. the more accurate.
Lauren is currently funded by an NHLBI K12 grant (1K12HL138049-01) studying the implementation of evidence-based diagnosis of pulmonary embolism in the emergencydepartment. She presents to the emergencydepartment with chest pain and some shortness of breath. Case: A 64-year-old woman with type-2 diabetes.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. Serial ECGs enhance the diagnosis of acute coronary syndrome. Annals of Emergency Medicine , 31 (1), 3–11. Leave it alone.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergencydepartment for evaluation of chest pain. 4) Lastly, the QRS amplitude in V2 (both the R- and S- waves) are measured.
Upon arrival at the receiving emergencydepartment, however, she precipitously degenerated into VF and could not be resuscitated. In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Unfortunately, a post-conversion 12 Lead was not acquired.
Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI.
But the bradycardia and the infero-posterior OMI is definitely new: Smith : this also has many abnormalities suggestive of ischemia: many leads have ischemic appearing ST depression The emergency provider followed the sequential steps of the current paradigm: 1.
When he showed it to me, I said "Ouch, looks like an acute coronary occlusion. no LBBB or paced rhythm), acute coronary occlusion MI (OMI) is diagnosed in approximately 75% of cases. The Smith-Modified Sgarbossa Criteria Accurately Diagnose Acute Coronary Occlusion in EmergencyDepartment Patients With Ventricular Paced Rhythm.
However, none of the formulas have proven to be definitively better than another and none are well correlated with outcomes or events! But the QT is definitely greater than half the RR interval. None is considered definitive due to the paucity of data (and conflicting data) relating QTc to outcomes. which is 0.6
Approach to Syncope Syncope definition: Brief loss of consciousness with loss of postural tone and complete spontaneous recovery without medical intervention. This San Fran definition, however, is too non-specific , so I list more specific ECG abnormalities below: b. 2) Boston syncope rule: J Emerg Med. 2007 Oct; 33(3): 233–239.
3,10 Coronary Allograft Vasculopathy Nicknamed “The Achilles Heel of Heart Transplantation,” this accounts for the majority of patient mortality in the 5-10 year range. 10 It affects the whole length of the vessel and all layers of the coronary vasculature rather than just the intima, which is seen in non-transplant atherosclerosis.
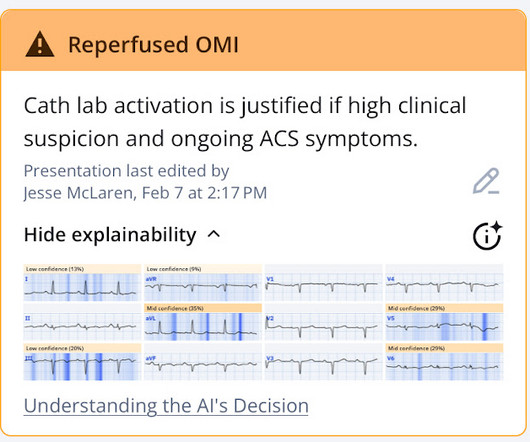
Annals of Emergency Medicine. PMID: 39066765 What They Did: The study involved the development of a deep ensemble AI model using ECG data from a prospective percutaneous coronary intervention registry in Korea. Two board-certified cardiologists reviewed and classified the ECGs, and their consensus served as the gold standard.
The use of CTA (computed tomography angiography) in the emergencydepartment (ED) has increased dramatically in the past 20 years. 63 This is because their definition of CI-AKI is an AKI that ensues within 48 hours of receiving IV contrast in the absence of any “other nephrotoxic factors.” Forman, H. Yaesoubi, R. 21.26543. (3)
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergencydepartment with chest pain. Also : See Ken Grauer's excellent comments at the bottom. He developed it only 20 minutes prior to presentation while cutting branches outside.
Written by Jesse McLaren An 80 year old with a history of CHF, ESRD on dialysis, and multiple prior cardiac stents presented to the emergencydepartment with 3 days of intermittent chest pain and shortness of breath that resolved after nitro, which felt like prior episodes of angina. So which was the culprit?
EMS gave aspirin and nitroglycerin, and the patient noted significant improvement on arrival to the EmergencyDepartment. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. Here is her ECG on arrival to the ED: Improved, but still some signal of posterior OMI.
While acute cutaneous lupus lesions are highly characteristic of SLE, subacute and chronic skin changes may occasionally develop in individuals without a definitive SLE diagnosis (1,5). SLE is considered an atypical risk factor for cardiovascular disease and acute coronary syndrome(8,9,11).
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. She presented to the EmergencyDepartment at around 3.5 She was emergently transferred to a PCI center. KEY Points: DSI does not indicate acute coronary occlusion!
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content