This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
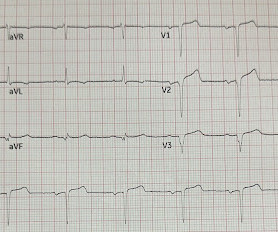
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. There is increased LV cavity dimensions with an increase in transient ischemic dilation, suggesting Left Main, or 3-vessel coronary artery disease. His spouse had called 911 after she heard a loud “thud” in the adjacent room.
We’ll keep it short, while you keep that EM brain sharp. Upon further research in the 1970’s, retrospective data from autopsies of those patients showed coronary aneurysms 5 Pathophysiology: Kawasaki Disease is a vasculitis of medium sized arteries.
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. Available from: [link] Guldner GT, Smith T, Magee EM.
EMS arrived and found him in Ventricular Fibrillation (VF). But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! This patient was witnessed by bystanders to collapse.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Hope you’re doing well! How excited would you have been about this case?" No Chest Pain, but somnolent.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. It’s judicious, then, to arrange for coronary angiogram. Supply-demand mismatch (non-occlusive coronary disease, or exacerbation of preexisting flow insufficiency) a.
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. This included the addition several new STEMI equivalents [4] on ECG that warrant “prompt evaluation for emergency coronary angiography.”
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. This is not the case.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
When EMS found her, she was dyspneic and diaphoretic. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. 1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay. Attached is the first ECG. Isn’t VT ALWAYS “wide”?
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. EMS arrived — and recorded 2 ECGs. 14 minutes later — ECG #2 was recorded by EMS. I personally can hardly wait for that future version! Some patients do this.
All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation. It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. All coronary arteries were patent without atherosclerotic change. To the uninitiated — this ECG may appear normal.
They are not premature, by definition. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g.
Extracorporeal membrane oxygenation Of patients with out-of-hospital cardiac arrest presenting to the ED in refractory VF, a majority have significant coronary artery disease, much of which is amenable to percutaneous coronary intervention. Circulation. 2019;139(12):e530-e552. Yannopoulos D, et al. J Am Coll Cardiol.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chest pain. Upon EMS arrival the patient appeared acutely ill and complained of chest pain. Other coronaries were normal. How do you interpret the ECG?
EMS arrived and recorded this ECG: What do you think? I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. So this study is worthless and must be ignored. Litell JM, Meyers HP, Smith SW.
She went to angio and had normal coronaries. No d-dimer or CT pulmonary angiogram was done when they discovered that she had normal coronary arteries. Think of this diagnosis when a patient with CP and SOB + elevated troponin — has normal coronary arteries on cardiac cath. I discussed all results with patient.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS.
When Pendell and I are coding ECGs for the Queen's training, this is one category: "Definite ischemia, difficult to differentiate between posterior OMI and subendocardial ischemia." The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. He was diagnosed as NSTEMI. Eur J Emerg Med.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. One need not have obstructive coronary disease to have occlusive thrombus!
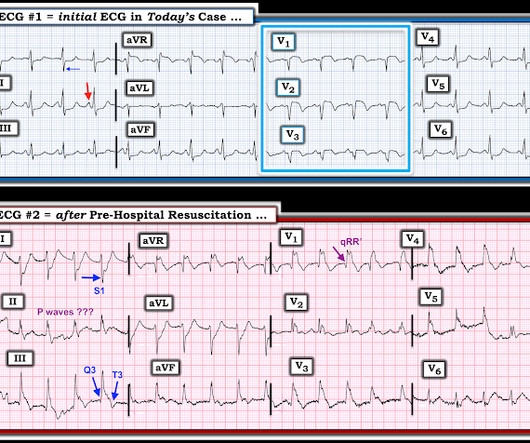
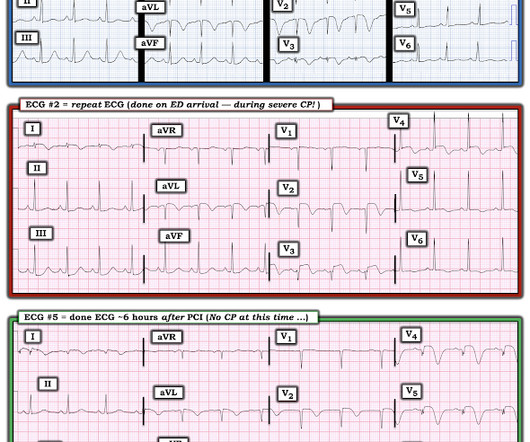
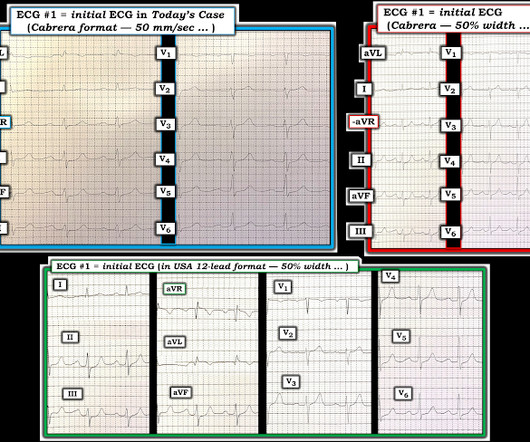
A Coronary angiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. Figure-1: The initial ECG in today's case — obtained by the EMS team. ( Regional wall motion abnormality- inferior and inferolateral. Why ECG #1 Looks Acute.
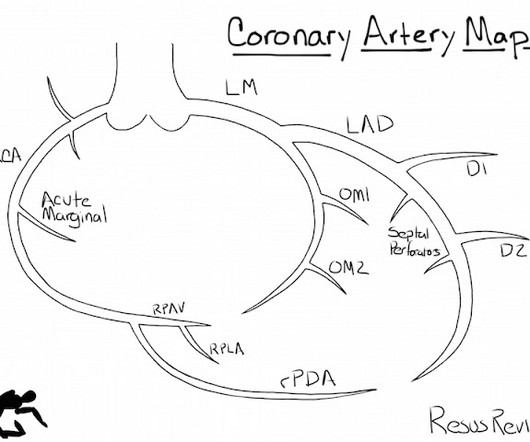
This illustration comes from Charles Bruen's great blog, Resus Review Coronary Artery Diagramming – Resus Review Charles is another illustrious graduate of the Hennepin EM Residency; actually, the EM/IM combined residency. Plus he did a 2 year combined EM Cardiology and Critical Care Fellowship.
The case below was contributed by Pendell Meyers, an EM G1 at Mt. Here is a link to the case report: Dynamic T-wave inversions in the setting of left bundle branch block Though Wellens' syndrome was described in the LAD territory, I have shown cases demonstrating that it occurs in any coronary distribution. Sinai though!) Limkakeng AT.
Open angle Closed angle Definitions Increased resistance to aqueous outflow through the trabecular meshwork. 790-819 EM docs: Central Retinal Artery Occlusion CanadiEM: Medical Concepts – Acute Angle Closure Glaucoma Post Created By: Anand Swaminathan MD, MPH Post Peer Reviewed By: Salim R. Bagheri 2015 ).
REBEL Core Cast 98.0 – AVNRT Click here for Direct Download of the Podcast Definition: A regular, narrow-complex rhythm with a ventricular rate that is typically > 160 bpm. Amal Mattu’s ECG Blog has an excellent review of AVNRT vs. VT and REBEL EM reviews the sensitivity and specificity of various algorithms.
Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Transient ST-segment myocardial infarction: a new category of high risk acute coronary syndrome?
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot.
EMS showed us their ECG on arrival at her house: What do you think? However, this STE is definitively abnormal in the setting of a normal QRS complex and hyperacute T-wave morphology in V2. The cardiologist arrived quickly and was skeptical about these findings on EMS ECG. We called for emergent cath lab activation.
So this ECG was immediately recorded: Indeed, as predicted, a patient with previous Wellens' waves who now definitely has chest pain has acute Occlusion, with new ST elevation in I, aVL, V2-V5. Since the patient has active pain now, if this is indeed Wellens,' she must be re-occluded at this moment. The Cath lab was activated.
In combination with the subtle ST depression in aVL , these changes are diagnostic for, or at least nearly so, for acute occlusion of a coronary artery, probably with some reperfusion, as inferior T-waves are inverted and the T-wave in aVL is reciprocally upright.
EMS arrived and found her in a wide complex PEA rhythm. The ultimate reason for the long QT was never definitively determined. Drug-induced QT interval cannot be completely ruled out, but the tox consult found the she had definitely not overdosed and did not believe that therapeutic doses would do this.
The patient contacted EMS after a few hours of chest pain that started 5:30 AM. There is slight but definite ST elevation with an inverted T wave in lead aVL. Eventually with more training the QoH will outperform any human in the detection of acute coronary occlusion. He is otherwise healthy.
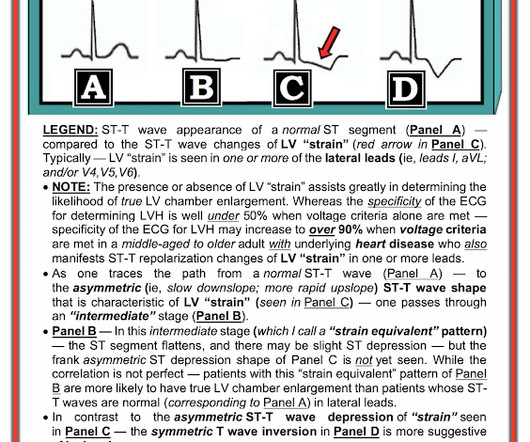
The QRS duration is 118 ms , so by definition it is not Left Bundle Branch Block (which must be 120 ms at a minimum and is usually longer) Thus, LVH on the ECG does not always correlate with anatomic LVH. Discussion Thus, no further ECGs were recorded and there was no angiogram or stress test or CT coronary angiogram. There is LVH.
Past medical history includes coronary stenting 17 years prior. Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. Read this post: Idiopathic Ventricular Tachycardias for the EM Physician 2.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. Serial ECGs enhance the diagnosis of acute coronary syndrome. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Bigger et al.
David Didlake, NRP, APRN, ACNP-BC @DidlakeDW Expert analysis provided by Dr. Ken Grauer [link] @ekgpress EMS is called to the main reception area of a retirement center where an elderly female is found down, unconscious and unresponsive. She has a palpable pulse at the radial arteries, bilaterally, with shallow respirations.
See the variety of Left Main Occlusion ECGs here: How does Acute Total Left Main Coronary occlusion present on the ECG? == MY Comment , by K EN G RAUER, MD ( 5/3 /2024 ): == Most patients with acute LMain Occlusion do not survive to make it to the hospital. Left Main Non-Occlusive ACS presents with widespread ST Depression and STE in aVR.
EMS found her acutely ill, mottled, dry mucous membranes, modestly hypotensive, and lethargic. They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. Example 1 EMS is called to the residence of an elderly male experiencing profound weakness. The serum K returned 8.7,
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). There is no definite evidence of acute ischemia. (ie, The below ECG was recorded.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
appeared first on REBEL EM - Emergency Medicine Blog. Background: Massive pulmonary embolism defined as sustained hypotension (SBP <90mmHg) has a high mortality which is why early recognition and thrombolytic therapy is typically recommended (AHA Class IIA; ESC Class IB) [1].
This is by one of our outstanding 3rd year residents , Aaron Robinson, with some edits and comments by Smith EMS responded to a reported seizure in a 42 year old male. One of our EMS Fellows along with a Senior EM Resident were on duty that evening, and arrived on the scene with the Fire Department.
Acute coronary occlusion is the most common and most treatable cause of this pattern, but it is not the only cause. Takotsubo, spasm, low flow with a preexisting stable coronary lesion, etc. The myocytes do not know why they are dying, they can only report their death and hope you can see it and figure it out.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content