This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
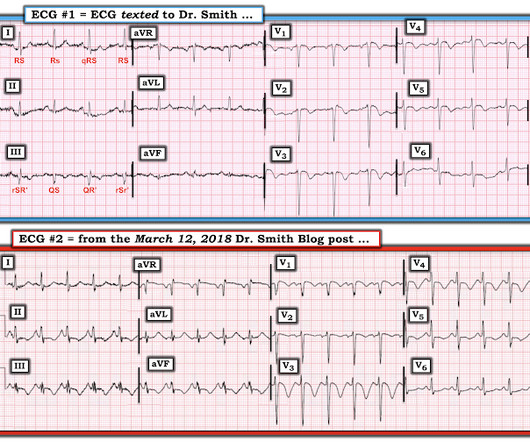
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
Triage documented a complaint of left shoulder pain. Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. In this version 1, the Queen of Hearts does not compare serial ECGs. At midnight.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. So maybe she is better than I am.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E.
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. LEARNING POINT : 1. Smith and Meyers containing thousands of tracings with documentation of cardiac catheterization results. in ECG #1 ). These were texted to me only with "chest pain."
It is true that other documents occasionally describe "abnormal ST segment elevation" in the posterior leads (commonly accepted criteria is 0.5 mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent."
4 important features that indicate acute right hear strain: 1. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with APE (p less than 0.001). They found that only 11% of PE had 1 mm T-wave inversions in both lead III and lead V1, vs. 4.6%
2020;71(1):235-246. Plt 37×10^9/L and 40×10^9/L, SOC and TEG, respectively) All patients enrolled had an upper endoscopy and verified the source of bleeding. Article: Kumar M et al. Thromboelastography-Guided Blood Component Use in Patients With Cirrhosis With Nonvariceal Bleeding: A Randomized Controlled Trial.
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Reference: Hirsch KG, Abella BS, Amorim E, et al; American Heart Association, Neurocritical Care Society. 2023 Dec 1.
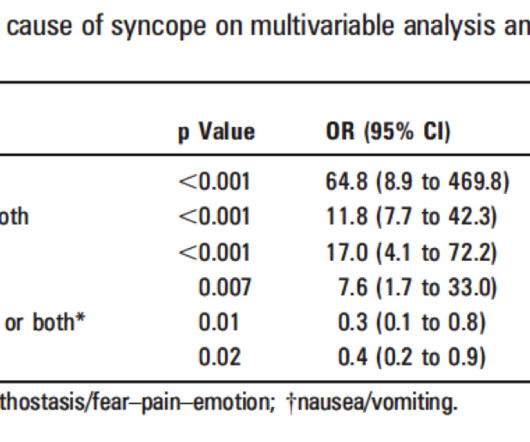
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. The arterial pressure waveform is transduced using the coronary catheter. But in the case of an ostial lesion, there is little or no space between the outside of the catheter and the wall of the coronary artery.
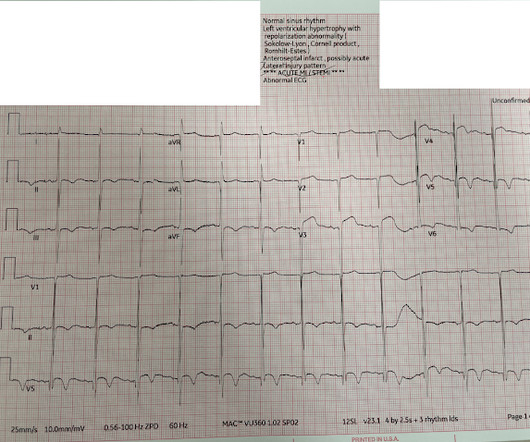
The emergency physician does cautiously (correctly) note that the ECG meets STEMI criteria in V3 and V4, but goes on to document absence of ACS symptoms. Pendell Meyers , Aaron E. PEARL #1: In general, it is rare to see both marked LVH and acute OMI in the same tracing. PEARL #2: The above said Remember the rule of "N = 1".
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content