This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
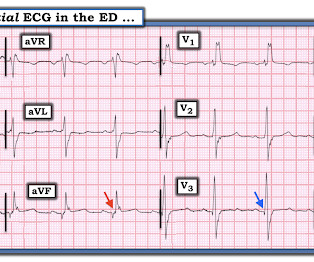
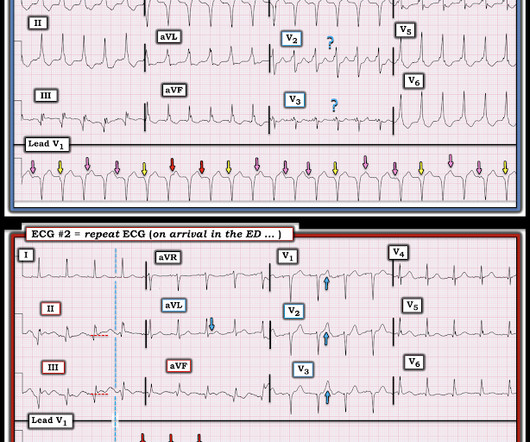
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Patient not informed of enlarged heart, dies 3 weeks post ED visit Miscommunicated radiology findings are a hot topic. Someone should have – either the first ED doc, the second ED doc, or my PCP.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
Past medical history includes coronary stenting 17 years prior. Initial ED ECG: What do you think? Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. How Can We Prove that ECG #1 is VT?
showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. In fact, Kosuge et al.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Triage documented a complaint of left shoulder pain. For the same reason, you should not delay coronary angiography because pain resolves with morphine. She contacted her neighbor, a nurse, for help.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). This patient presented to the ED “after a couple of days of chest discomfort”. Remember that this patient presented to the ED “after a couple of days of chest discomfort”.
EKG on arrival to the ED is shown below: What do you think? The providers documented concern for ST elevation in the precordial and lateral leads as well as a concern for hyperkalemic T waves in the setting of succinylcholine administration. or basilar ischemia. However, T waves do not appear to be hyperacute or hyperkalemic.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Figure-1: The initial ECG that was done in the ED ( See text ).
6] Among 394 emergency department Code STEMI patients with acute culprit lesion requiring coronary interpretation, 16 (4.1%) presented with an ECG labeled ‘normal’ or ‘otherwise normal’ by computer interpretation. have published a number of warnings about the previous reassuring studies.[4,5] minutes).
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic. Akkerhuis KM, et al.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. In the ED, his troponin, ECG, and chest X-ray (CXR) are normal. Then what? He survives.
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergency department (ED). This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Then this was recorded in the ED 10 minutes after the first: Now there is massive STE Many inferior MI are associated with RV MI. BOTTOM — 2nd ECG obtained 10 minutes later in the ED ( See text ). She called 911.
STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. the presence of J waves from early repolarization doesn’t rule out an acute coronary occlusion 4. Am J Emerg Med 2023 2.
On arrival to the ED, the patient was diaphoretic, tachycardic. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? I was not worried for a coronary etiology. He had a prehospital ECG that was worrisome to the medics, so they called me to see him at the door. and had dilated pupils.
T he C ASE : The patient is a 60-something who presented to the ED with n ew- o nset c hest p ain. K EY P oints : This patient has known coronary disease. In this patient with documentedcoronary disease — these q waves could reflect prior lateral infarction ( especially in view of the Q in lead aVL ). It was stented.
Emergent CT coronary angio also likely has a role in such cases. Like they would for any other acute arterial occlusion syndrome (such as suspicion of acute large vessel stroke), they take the patient across the hall and perform an immediate CT (coronary) angiogram, showing patent coronaries.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative. Setting – large, academic, suburban ED. CT aorta negative for dissection.
To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted. Figure-1: Comparison between the first 3 ECGs in today’s case. What We Learn from the Prior Tracing?
The P wave is positive in lead aVL of ECG #3, which means it is a low atrial (or probably coronary sinus) rhythm — which of itself is not necessarily “abnormal” in a child if there is no other sign of underlying heart disease. As we see in ECG #3 — the regular rhythm is NOT sinus, because the P wave is negative in lead II.
A middle-aged man presented with 7-8/10 non-radiating chest tightness to the left chest wall, associated with nausea but no diaphoresis, that began while walking approximately 40 minutes prior to arrival at the ED. He was definitely pain free by the time of arrival at his ED room. What do you think? Chest Pain scores can be misleading.
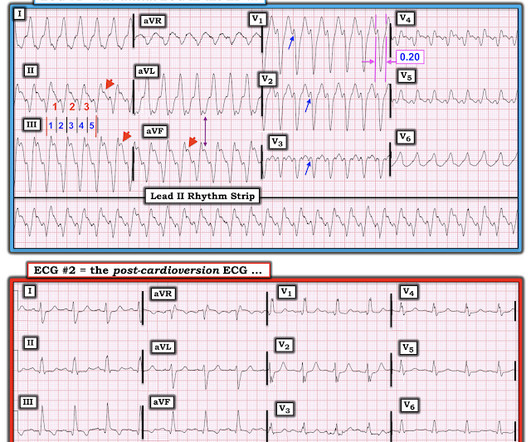
An elderly woman with history of coronary disease presented with CP and SOB and hypotension by EMS. Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. The patient was given a small dose of etomidate and electrically cardioverted in the ED.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. link] An angiogram was done: It showed no culprit and no coronary disease, but did show a myocardial bridge in the mid LAD.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergency department (ED) for an electrical injury and fall from a high voltage electrical pole. Acute myocardial infarction with normal and near normal coronary arteries. Electrical Injuries. 2023 Jul 17. In: StatPearls [Internet].
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 He denied chest pain or shortness of breath. See below for PM Cardio digitized version of this.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chest pain described as an “explosion" of left chest pressure. At the time of arrival to the ED, the patient reported 1/10 chest pain with normal vital signs. Triage EKG: What do you think?
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
The 2 clinical areas of most potential benefit to emergency care from computerized interpretations are: i ) Cardiac arrhythmias; and , ii ) Rapid detection of acute coronary O cclusion ( ie, detection of acute O MI ) in cases for which easily recognizable STEMI-criteria are not present. What About the Initial ECG?
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin.
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. We performed a beside US (shown below) which showed lateral wall hypokinesis as read by an US-boarded ED attending in real time. 418 of these 1788 (23%) had acute coronary occlusion.
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS."
They gave him 2 nitroglycerine and transported to the ED. In the ED, the patient was "moaning, writhing in bed, and clutching his chest." Here is the first ED ECG (there was no previous ECG on file for comparison): Sinus rhythm and LVH There is some (less than 1 mm) of STD in V3 and V4. There is no significant ST Elevation.
This is a re-posting of a Tweet by Robert Jones (@RJonesSonoEM), reproduced with permission, written by Pendell Meyers A middle aged female with history of smoking presented to the ED with "bad heartburn." Here is her prior baseline ECG (first), and her ED ECG (second): Baseline: ED ECG: What do you think?
Smith and Meyers containing thousands of tracings with documentation of cardiac catheterization results. Along the way to acquiring more experience in recognizing the ECG findings of acute coronary occlusion — is incorporation of a number of KEY ECG Features into one's clinical acumen.
It is true that other documents occasionally describe "abnormal ST segment elevation" in the posterior leads (commonly accepted criteria is 0.5 mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent."
The medicine note documents that the patient had worsening pain with lying flat and relief with leaning forward. Upwardly Concave ST Segment Morphology Is Common in Acute Left Anterior Descending Coronary Artery Occlusion. Myocarditis is virtually indistinguishable in the ED from MI. 2 comments : 1. 0 0 1 24 140 MMRF 1 1 163 14.0
Here is his ED ECG: There is obvious infero-posterior STEMI. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." Over a 13-month period, serum potassium and magnesium levels were measured in 590 patients admitted to a coronary care unit. He appeared to be in shock.
According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. paramedic transportation to the ED as “chest pain, STEMI negative” 2. Take home 1. Eur Heart J 2019 5.
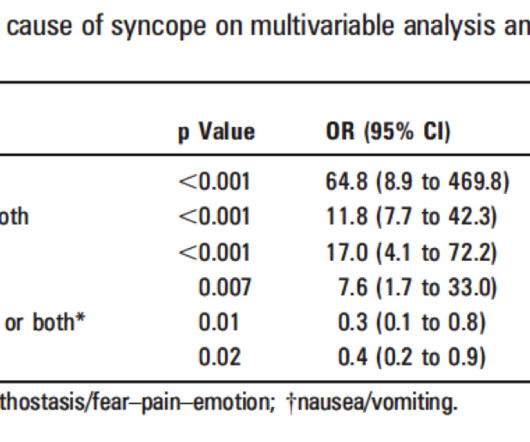
Summary of ED Approach to Syncope Please excuse the formatting problems, which I have not been able to fix! Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful. Any ED systolic blood pressure less than 90 or greater than 180 mm Hg (+1) 4.
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. KEY Points: DSI does not indicate acute coronary occlusion!
Documentation lists a diagnosis of "sinus tachycardia." The patient was then sent to the ED for evaluation not by ambulance but driven to the ED by his wife. Finally Dr. Frick details how today's patient was found to have severe, stable coronary disease without evidence of an acute event. He was admitted to cardiology.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content