This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. Autopsy shows coronary atherosclerosis and marked cardiomegaly with a thickened left ventricular wall. It wasn’t, so you weren’t called, nor did the doc need to document anything. Baccei SJ et al.
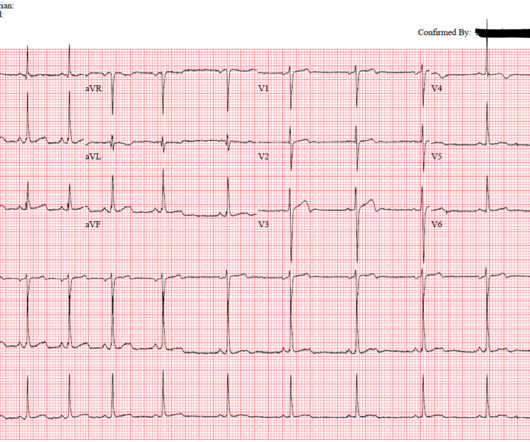
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. What do you think?
American College of Cardiology released a new consensus statement, “ Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the EmergencyDepartment: A Report of the American College of Cardiology Solution Set Oversight Committee “. J Am Coll Cardiol. 2022 Nov 15;80(20):1925-1960.
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment. Am J Emerg Med.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Written by Bobby Nicholson What do you think of this “STEMI”? Blood glucose was not low at 162 mg/dL.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergencydepartment for evaluation of chest pain. 4) Lastly, the QRS amplitude in V2 (both the R- and S- waves) are measured.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Guagliumi, G., Iwaoka, R.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. He had no previously documented medical problems except polysubstance use. Annals of Emergency Medicine , 31 (1), 3–11.
She presented to the emergencydepartment after a couple of days of chest discomfort. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). The last echocardiography 12 months ago showed HFmrEF. The ECG below was recorded.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. 1 Opioids or anxiolytics are often given to patients whose diagnosis of AD is missed or delayed.
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergencydepartment (ED). 1 Despite the rarity of dextrocardia, coronary artery disease can occur with a similar frequency to that of the general population.
It was ongoing on arrival in the emergencydepartment. STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. Below is the old ECG (on top) and then new ECG (on bottom).
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. Electrical injuries in the emergencydepartment: an evidence-based review. Emerg Med Pract.
The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. The patient was transferred to the PCI center non-emergently over the next few hours.
Because the patient's pain had resolved completely and cardiology had declined immediate intervention, the patient was admitted but continued to board in the emergencydepartment. Approximately 4 hours after arrival, the patient was re-examined by the emergency physician. The iStat POC assay is 0.08
The pain resolved as he arrived to the emergencydepartment. Even if troponins are negative and infarction is not documented — dynamic ECG changes in association with new chest discomfort is indication for investigation. He had 2 episodes over the past 2 days of similar chest tightness. Chest Pain scores can be misleading.
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e I B Patients transferred to PCI centres can bypass the emergencydepartment to undergo primary PCI without delay. STEMI , ST-segment elevation acute myocardial infarction ).
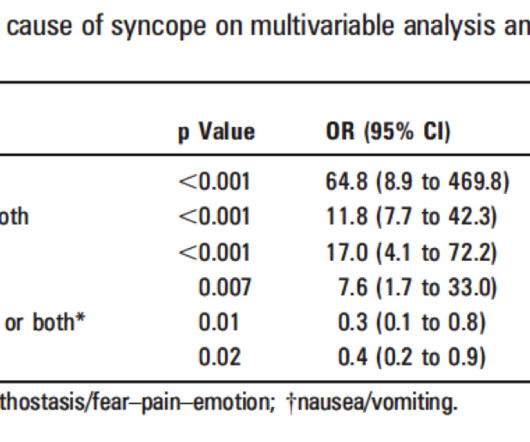
Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful. 2) Boston syncope rule: J Emerg Med. The ROSE (Risk Stratification of syncope in the emergencydepartment) Study. 2007 Oct; 33(3): 233–239.
According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Cardiology documented “late presentation STEMI but likely aborted given resolution of ST changes from EMS to hospital.”
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. She presented to the EmergencyDepartment at around 3.5 She was emergently transferred to a PCI center. KEY Points: DSI does not indicate acute coronary occlusion!
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergencydepartment with chest pain. Also : See Ken Grauer's excellent comments at the bottom. He developed it only 20 minutes prior to presentation while cutting branches outside.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content