This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
Dr. Smith and other authors showed the utility of Speckle Tracking Strain Echo in this case report: Diagnosis of acute coronary occlusion in patients with non–STEMI by point-of-care echocardiography with speckle tracking Repeat ECG: Slightly less hyperacute T waves, likely indicating improving flow compared to the first ECG.
And you can see why: the artery may sponstaneously reperfuse, as it did here well before angiography, and documented with resolution of pain and evolution of the ECG to typical full reperfusion pattern Peak troponin I was 8544 ng/L. This is diagnostic of full reperfusion.] 90% of normals have some STE in V2 and V3. Which 1 or 2 leads are KEY?
An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. Autopsy shows coronary atherosclerosis and marked cardiomegaly with a thickened left ventricular wall. It wasn’t, so you weren’t called, nor did the doc need to document anything.
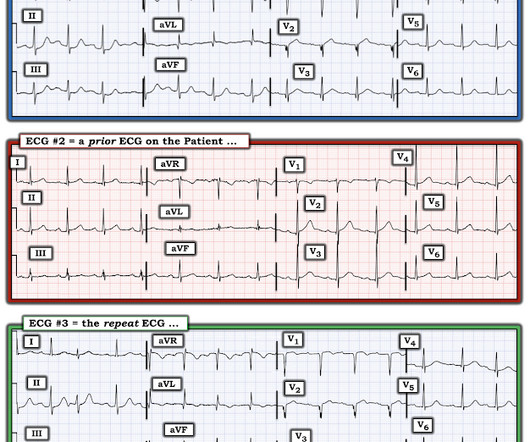
The most likely would be #2) initially normal, then #3) subtle OMI, then #4) obvious STEMI, and then #1) reperfusion: In other words, the patient with an initially normal ECG develops an acute coronary occlusion, with ECGs that progress from subtle to obvious, and then reperfuse after angiography. 2 Normal ECG #3.
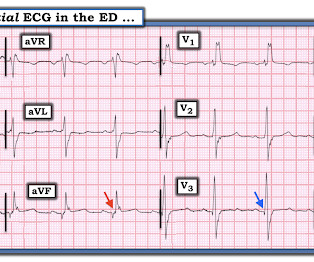
Past medical history includes coronary stenting 17 years prior. Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. Initial ED ECG: What do you think? Why did I say that?
This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents. STEMI vs. NSTEMI dichotomy is not sensitive for true occlusion MI or acute coronary occlusion. NCSE is likely more common than we think.
Triage documented a complaint of left shoulder pain. For the same reason, you should not delay coronary angiography because pain resolves with morphine. The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. The patient presented to triage at around 10 PM.
showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. In fact, Kosuge et al. Stein et al.
The providers documented concern for ST elevation in the precordial and lateral leads as well as a concern for hyperkalemic T waves in the setting of succinylcholine administration. Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronary artery disease.” (!!!) or basilar ischemia.
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
You can easily imagine this patient getting one of several diagnoses -- vasospasm, MINOCA , pericarditis, or maybe even no diagnosis at all beyond "non-obstructive coronary artery disease." Another option would be to use Optical Coherence Tomography for Coronary Imaging ). That plaque is at risk of thrombosing again.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The following ECG was obtained. ECG 1 What do you think?
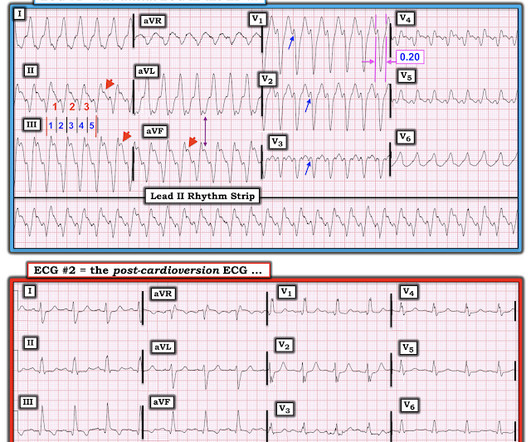
The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. Is this: 1. In either case, prompt cardioversion is indicated.
6] Among 394 emergency department Code STEMI patients with acute culprit lesion requiring coronary interpretation, 16 (4.1%) presented with an ECG labeled ‘normal’ or ‘otherwise normal’ by computer interpretation. Written by Jesse McLaren Four patients presented with chest pain. minutes).
in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47 in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47 in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47
He had no previously documented medical problems except polysubstance use. Serial ECGs enhance the diagnosis of acute coronary syndrome. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the Crusade Quality Improvement Initiative. Perform serial ECGs even if symptoms are constant.
His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Chest pain is documented as ongoing. Repeat 0157 with ongoing chest pain: Basically the same features diagnostic of LAD occlusion. QOH: "OMI High confidence". Physician interpretation: "No STEMI."
It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi). Akkerhuis KM, et al.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. the presence of J waves from early repolarization doesn’t rule out an acute coronary occlusion 4.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. 1 Opioids or anxiolytics are often given to patients whose diagnosis of AD is missed or delayed.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The more leads in a given lead area that show hyperacute changes — the greater the concern for acute OMI.
We assume that at some point the patient's pain returned, but it is not documented, so exactly when this happened is uncertain. Immediately after the second ECG was performed, the patient's pain resolved completely. After reviewing the case, cardiology requested that the patient be admitted to observation for stress testing the next morning.
This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries. 1 Despite the rarity of dextrocardia, coronary artery disease can occur with a similar frequency to that of the general population. Coronary heart disease in situs inversus totalis.
Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. As he documented, “This patient is experiencing chest pain consistent with an acute coronary syndrome. As cardiology documented, “possible STEMI. Start using the terms acute coronary occlusion and occlusion MI. Q wave, old infarct?
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. K EY P oints : This patient has known coronary disease. It was stented. But 1% may be/have neither!
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. He denied chest pain or shortness of breath. PM Cardio digitized version.
I was not worried for a coronary etiology. Possible explanations include: i ) Coronary vasospasm, with a brief period of coronary occlusion; ii ) Supply-demand mismatch ( Type II MI ) — precipitated by amphetamine-induced catecholamine surge; and / or , iii ) Catecholamine-mediated platelet aggregation with subsequent thrombus formation.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative. Repeat ECG: New developing Q waves in V2 and V3, further confirming evolving OMI.
But it does prove that the patient has coronary disease and makes the probability that his chest pain is due to ACS very very high. Instantaneous wave-free ratio is performed using high fidelity pressure wires that are passed distal to the coronary stenosis. We need to do some more investigation.
Emergent CT coronary angio also likely has a role in such cases. Like they would for any other acute arterial occlusion syndrome (such as suspicion of acute large vessel stroke), they take the patient across the hall and perform an immediate CT (coronary) angiogram, showing patent coronaries. I immediately responded: "cool fake!
To realize — Assessment of ECG #1 is complicated by knowing: i ) That today’s patient has a history of documented CAD ; and , ii ) The lack o f a prior tracing for comparison at the time the initial ECG was interpreted. The interventionalist asked for another troponin, which shortly returned at 66 ng/L. What We Learn from the Prior Tracing?
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. The condition of the coronary artery at the time of angiogram may be different than it was 30 minutes prior during recording of the ECG. A 40-something woman had sudden chest pain. She called 911. The proposed mechanism is complex.
link] An angiogram was done: It showed no culprit and no coronary disease, but did show a myocardial bridge in the mid LAD. An excellent review of myocardial bridging, with full text: [link] Myocardial bridging is when the coronary artery, usually the LAD, dives into the myocardium.
Thick, dry, and calloused skin of a construction worker can have as much as 100 times more resistance than the previous example. 4 This may lead to more heat dissipated at the skin with impressive burns to skin, but less transmission of electricity to deeper tissues. High voltage” is defined by texts as 600 V and 1,000 V. Click to enlarge.)
The P wave is positive in lead aVL of ECG #3, which means it is a low atrial (or probably coronary sinus) rhythm — which of itself is not necessarily “abnormal” in a child if there is no other sign of underlying heart disease. As we see in ECG #3 — the regular rhythm is NOT sinus, because the P wave is negative in lead II.
An elderly woman with history of coronary disease presented with CP and SOB and hypotension by EMS. Angiogram: Severe coronary artery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronary artery disease.
After admission he undergoes another ECG, though it is unclear from documentation whether there was a change in his chest pain. Documentation strongly suggests that this finding was what ultimately convinced the cardiologists that this was not pericarditis. After this result he was given therapeutic enoxaparin. Teaching points: 1.
The 2 clinical areas of most potential benefit to emergency care from computerized interpretations are: i ) Cardiac arrhythmias; and , ii ) Rapid detection of acute coronary O cclusion ( ie, detection of acute O MI ) in cases for which easily recognizable STEMI-criteria are not present. But beware when it makes these calls.
Even if troponins are negative and infarction is not documented — dynamic ECG changes in association with new chest discomfort is indication for investigation. He had a history of hypertension but stopped taking his medication several years ago. The patient is pretty sure that this discomfort was his reflux. BP was 200/100. What do you think?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content