This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
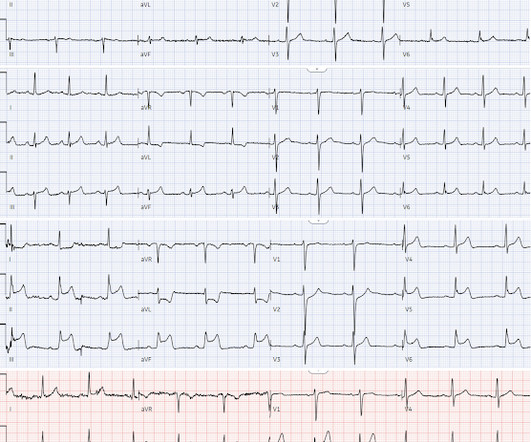
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. He was started on nitro gtt.
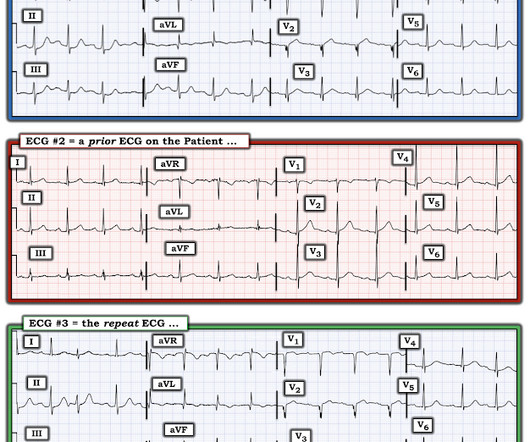
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? When the pain recurred the ECG normalized(ECG#2), but this is pseudonormalization : the coronary artery has spontaneously reoccluded, and the T waves are on their way up. What was the outcome and final diagnosis?
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
Triage documented a complaint of left shoulder pain. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." But pain is a critical signal for urgency in the context of acute coronary syndrome.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 which is concerning for LAD occlusion.
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. And you can see why: the artery may sponstaneously reperfuse, as it did here well before angiography, and documented with resolution of pain and evolution of the ECG to typical full reperfusion pattern Peak troponin I was 8544 ng/L. What did I say?
He had no previously documented medical problems except polysubstance use. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Serial ECGs enhance the diagnosis of acute coronary syndrome. Is there STEMI? An ECG was obtained shortly after arrival: What do you think?
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). In both tracings — an exceedingly fast PMVT is documented. The below ECG was recorded. He was taken immediately to the cath lab.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. In fact, Kosuge et al. Accessed May 28, 2024.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries. Figure 1: EKG for Dextrocardia showing STEMI. The second EKG was concerning for STEMI in the precordial leads (see figure 1). Click to enlarge.) 1 It has a prevalence of 0.01
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e STEMI , ST-segment elevation acute myocardial infarction ). I B Ambulance personnel must be trained and equipped to identify STEMI and administer fibrinolysis if necessary.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." We know that even high-sensitivity troponin may not exceed the "normal" range for a period of hours in certain patients with acute coronary occlusion. The following ECG was obtained.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Repeat ECG: New developing Q waves in V2 and V3, further confirming evolving OMI.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. To me, that is a meaningless diagnosis. Here is the main learning point: The infarct was due to an occluded artery (Occlusion MI, OMI). In 30% of OMI, there is no significant ST Elevation.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. The condition of the coronary artery at the time of angiogram may be different than it was 30 minutes prior during recording of the ECG. She called 911. But which myocardial walls are affected? The proposed mechanism is complex.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria. This was sent to me by a friend.
Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Learning Points: This is one of many examples of false positive STEMI criteria, which is distinguishable by expert humans, and now by AI such as QOH. Emergent CT coronary angio also likely has a role in such cases.
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician interpretation: "No STEMI."
Meyers note: notice in their documentation many of the classic mistakes of the STEMI generation: "Non ST Elevation MI" as their reasoning for why the patient did not merit emergent reperfusion, while simultaneously calling it "emergently" (after 8 hours!!!) Because we are hypnotized the STEMI paradigm. "If
After admission he undergoes another ECG, though it is unclear from documentation whether there was a change in his chest pain. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
The P wave is positive in lead aVL of ECG #3, which means it is a low atrial (or probably coronary sinus) rhythm — which of itself is not necessarily “abnormal” in a child if there is no other sign of underlying heart disease. Is there STEMI? AIVR is NOT common in otherwise healthy children. What is it? What is the rhythm?
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. So maybe she is better than I am.
Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial. These conversations should occur frequently and be clearly documented for other health care professionals who are not present during the conversations (96%, 22/23).
We assume that at some point the patient's pain returned, but it is not documented, so exactly when this happened is uncertain. Practice putting the probe on the chest of someone with an obvious STEMI(+) OMI in order to look for regional wall motion abnormalities. Clinical concern and gestalt should ultimately guide management.
The triage ECG was interpreted correctly as "No STEMI." This finally prompted a repeat ECG at 1341: 1350: Obviously STEMI(+) OMI. Compared to baseline, there is more STE in anterior leads, and significantly increased area under the curve of the T wave in V3 and V4. The second troponin returned higher at 45 ng/L.
Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion. Even if troponins are negative and infarction is not documented — dynamic ECG changes in association with new chest discomfort is indication for investigation. We assumed this was Wellens' syndrome and treated as such.
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. This is a high troponin (most STEMI are above 10 ng/mL for troponin I). Complete, bubble contrast echo is excellent: if there is no wall motion abnormality then it is very unlikely that there is a large epicardial coronary occlusion.
Take home messages: Any coronary occlusion may present with vague symptoms, but when ECG is clear, there should not be any suspicion. Fortunately, peak troponin was only 1090 ng/L and next day EF was 45-50% with apical and mid anterior hypokinesia. ECG hardly ever tells lies! Smith's Blog show this same phenomenon ).
The medicine note documents that the patient had worsening pain with lying flat and relief with leaning forward. Upwardly Concave ST Segment Morphology Is Common in Acute Left Anterior Descending Coronary Artery Occlusion. See this case: Pericarditis, or Anterior STEMI? There was no history of preceding viral symptoms.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
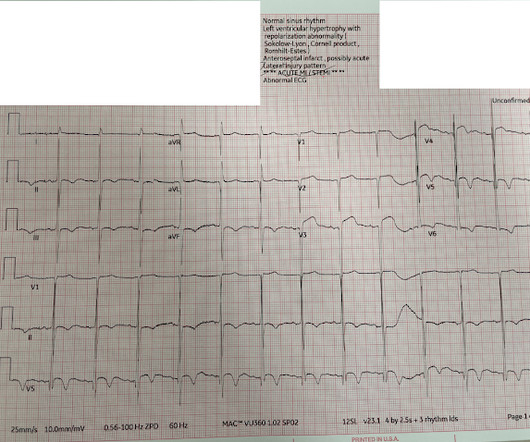
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. There were 80 positives by STEMI criteria, 88 by device algorithm, and 77 by AI software.
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." The ECG remains positive for STEMI by GE. Several hours passed with no documentation as to the reason for delay. In fact, even the GE algorithm got this one (partially) right.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content