This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
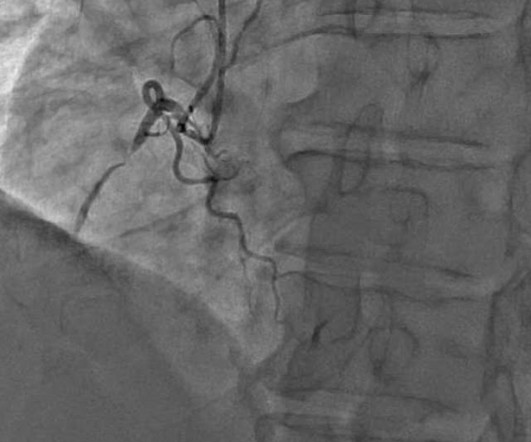
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. IMPRESSION: 1. Stroke-volume:50 ml.
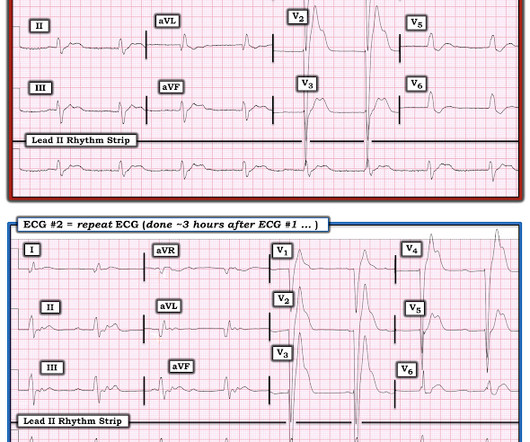
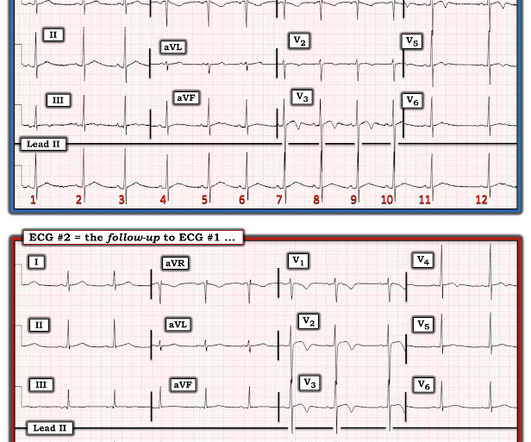
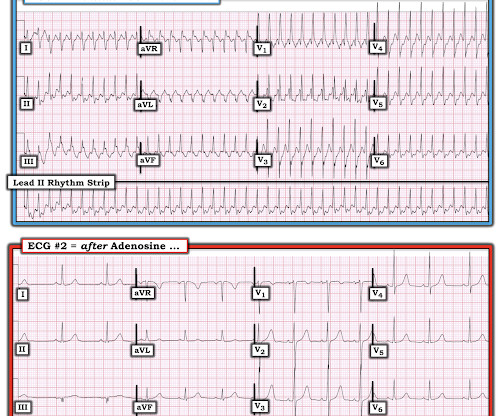
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Coronaries were clean. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. Time is myocardium.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
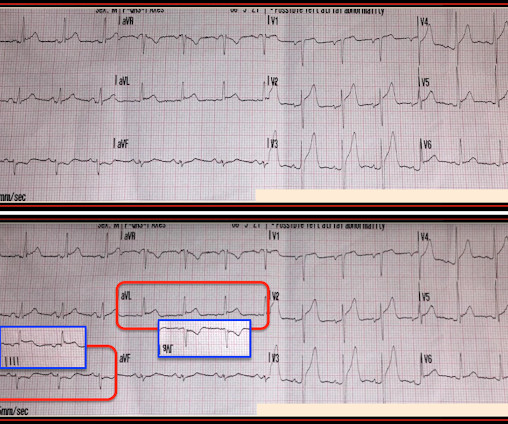
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. While not completely ruling out acute coronary disease — another cause should be considered.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. Learning Point: 1.
Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration.
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. 1 Risk Factors: 1-4 Spontaneous Anticoagulants (Apixaban, Rivaroxaban, etc.)
” – Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula). 3 A study of CT use trends in the ED has shown increasing use of CTs by almost 60% from 2005 to 2013.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Here is his ED ECG: There is bradycardia with a junctional escape. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. He appeared gray in color, with cool skin.
mg/dL (sorry, Europeans, for the weird units) Here was the initial ED ECG: There is a junctional rhythm with retrograde P-waves (see the dip in the T-wave in lead II across the bottom; you can follow that up to all the other leads and see the retrograde P wave). Learning Points: 1. Figure-1: The first 2 tracings in today's case.
Vittinghoff, E. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. The prohibition against beta blockade in cocaine toxicity, causing "unopposed alpha" stimulation, needs to be re-examined. is intuitive, and not surprising.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Setting – large, academic, suburban ED. Figure-1: The initial ECG in today's case.
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. I’ve excerpted in Figure-1 , relevant paragraphs from a 2017 ESC ( European Society of Cardiology ) article on this subject by Xanthopoulos & Skoularigis ( ESC: Vol. 15-9/6/2017 ).
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. What do you think?
He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent.
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. LEARNING POINT : 1. Along the way to acquiring more experience in recognizing the ECG findings of acute coronary occlusion — is incorporation of a number of KEY ECG Features into one's clinical acumen.
The coronaries were clean (this is not the gold standard, however, as some patients with ischemic ST elevation may have clean coronaries). ACTUAL CORONARY ANATOMY: Dominance: Right LM: A 5 mm vessel which bifurcates into the LAD and LCx coronary artery. QRSV2 = 16 RAV4 = 14 Value = 20.24 (The cutoff of 18.2
mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent." It's an ECG manifestation of transmural MI from an occluded coronary artery registered in the ECG leads FACING the infarcted ventricular wall.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chest pain and shortness of breath after finishing a 4-mile run. At the time of evaluation in the ED, his symptoms were resolved. Ct coronary angiogram showed normal coronary arteries.
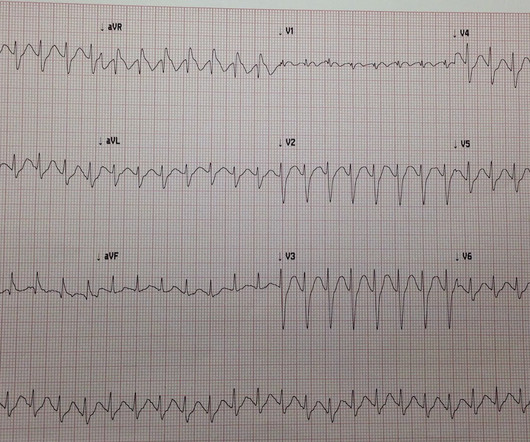
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. Tips for recognizing Acute Posterior STEMI: 1. References: 1. This can help in confirmation.
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. 25] Stone et al found that 72% have TIMI 0 or 1 flow.
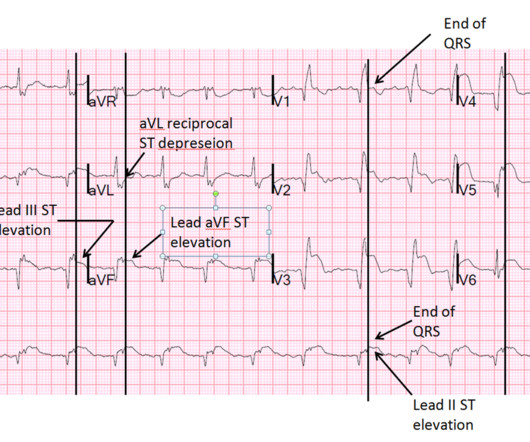
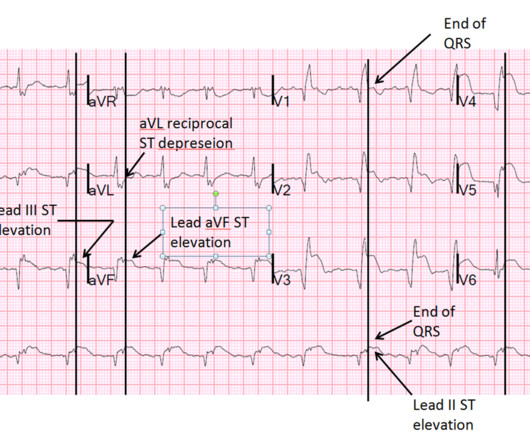
Is this due to coronary occlusion? The medic activated the cath lab but was refused by the interventionalist, who did not believe that this ECG represented acute coronary occlusion. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Why did I say this? Look at aVF.
A 30-something was in the ED for some minor trauma when he was noted to have a fast heart rate. See Learning point 1 below. They usually lasted anywhere between 1-2 hours. Here is the Electrophysilogist's note: "Only 1 pathway attachment could be ablated, the second one deep within the CS could not be ablated with high power.
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. We help you translate this to your clinical practice, by illustrating with a case.
We obtained access and monitoring, but she showed no signs of improvement, and we judged that an intervention must be done in the ED without delay. The ED catheter was removed at that point and she did not require any further procedures. Ultimately, she spent several days in the hospital and no further fluid collected.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. At midnight.
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. per year incidence of SCD in this cohort [1].
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable.
He had walked into the ED (did not use EMS). Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Our own Dave Plummer of HCMC reported on survival of 2 of 6 patients with free wall myocardial rupture diagnosed by bedside ultrasound in the ED.(3) J Am Coll Cardiol 53(17):1503-9.
He had walked into the ED (did not use EMS). Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Our own Dave Plummer of HCMC reported on survival of 2 of 6 patients with STEMI who had free wall myocardial rupture diagnosed by presence of hemopericardium on bedside ultrasound in the ED.(3)
Jafar Mahmood, MD (Pain Medicine Attending, Paincare Medical Practice) // Reviewed by: Jessica Pelletier, DO, MHPE (EM Attending, APD, University of Missouri-Columbia), Marina Boushra, MD (EM-CCM Attending, Cleveland Clinic); Brit Long, MD (@long_brit) Introduction: Pain management in the ED can be a unique challenge.
She describes the pain as left-sided, non-radiating, and 9/10 in severity. The catheterization lab is activated, but catheterization shows no coronary artery occlusion. A 67-year-old female with past medical history of hypertension presents with acute onset of chest pain without associated symptoms. What is the diagnosis?
A 64-year-old male presents by EMS to the ED with shortness of breath. 1 There are over 50,000 visits related to heart transplant in the United States each year and over half of these patients are admitted to the hospital from the ED. We’ll keep it short, while you keep that EM brain sharp.
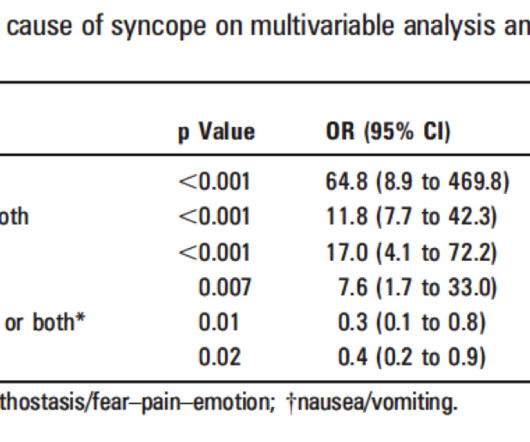
Summary of ED Approach to Syncope Please excuse the formatting problems, which I have not been able to fix! Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. Abnormal ECG – looks for cardiac syncope.
The use of CTA (computed tomography angiography) in the emergency department (ED) has increased dramatically in the past 20 years. 1 One study found that CTA head and neck was ordered for 2.5% of all patients in the ED for over 800 different stated indications. In a study of 17,903 CTAs ordered in the ED, Tu et al.
Whether your program is primarily 9-1-1, interfacility transport (IFT), or a combination of both, the likelihood of being responsible for the safe and expeditious transport of a STEMI patient is high for anyone in the out-of-hospital care setting. There, we would find two coronary ostias, left and right. Sir Isaac Newton.
A 43-year-old male with a history of mitral valve regurgitation s/p valvular replacement, hypertension, hyperlipidemia was evaluated in the ED for septic shock secondary to a pyelonephritis with a renal abscess. Chu CK, Delia E, Mograder A, Dwyer EM. 2017;45(1):12-20. 2015;7(9):E365-E369. 2018;12(1). J Thorac Dis.
Although these autoantibodies may be present in a variety of individuals, the development of clinical disease is thought to require exposure to an environmental risk factor such as certain viruses, cigarette smoke or other environmental toxins (1). million have been diagnosed with lupus, with 90% of cases occurring in females (1).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content