This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or EmergencyDepartment Assessment of Chest Pain (EDACS) score. Time to know your hs-cTn better.
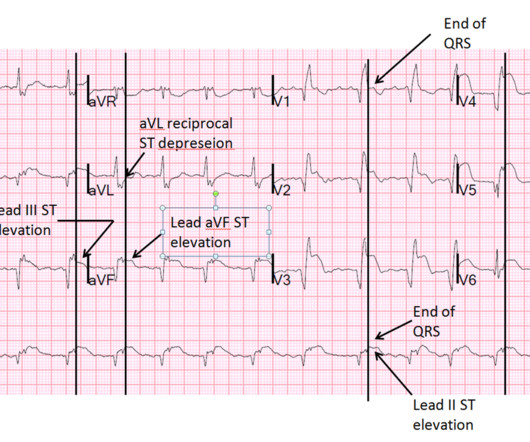
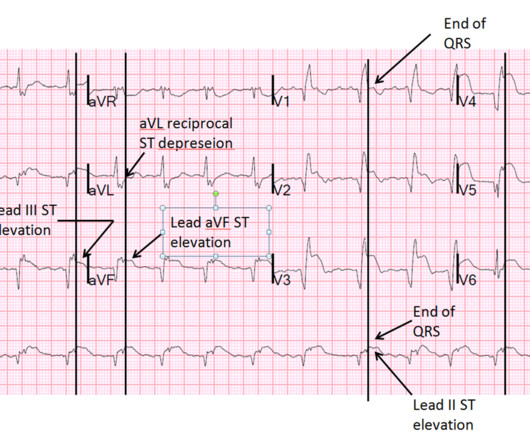
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage.
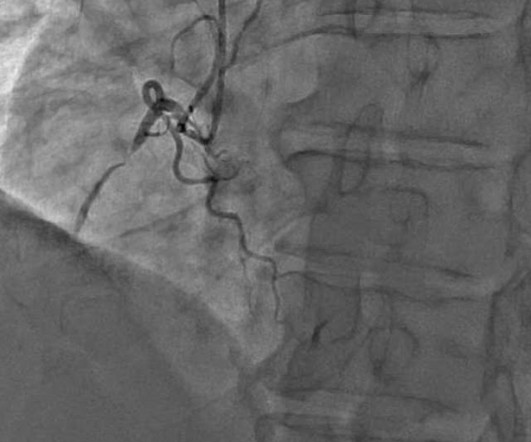
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think?
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
1 The shortage in supply posed difficulties for hospitals that significantly depend on GE Healthcare as their supplier, which encompassed approximately 50% of hospitals in the United States (US). 11 Table 1. Preparation 9 Hospitals had to prepare for the impending contrast shortage as soon as potential shortage news occurred.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion.
The patient’s ECG on arrival at the emergencydepartment is shown below. He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. For clarity — I’ve put these 2 tracings together in Figure-1.
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Baseline Q-wave surpasses time from symptom onset as a prognostic marker in ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention. J Am Coll Cardiol 53(17):1503-9. Very unlikely.
And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. In acute MI, the T-wave is large, and the T/ST ratio is high. This is much more typical of myocarditis.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. Pol Arch Intern Med. 2017;127:401–411.
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. He found 2 ECG patterns of atypical T-wave development in PIRP: 1) persistently positive (upright) T-waves 48 hours after AMI onset. Lessons : 1. Although rupture has a high mortality, it is not uniformly fatal References 1.
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Kirkegaard H, Soreide E, de Haas, I et al. De Fazio C, Skrifvars MB, Soreide E et al. 2019;23(1):1–9.
1 Indications for transplant include: Non-ischemic cardiomyopathy (49%) Ischemic cardiomyopathy (35%) Restrictive cardiomyopathy (4%) Retransplantation following failed prior transplant (3%) Hypertrophic cardiomyopathy (3%) Congenital heart disease (3%) Valvular cardiomyopathy (3%) The median survival after heart transplant is over 12 years.
The use of CTA (computed tomography angiography) in the emergencydepartment (ED) has increased dramatically in the past 20 years. 1 One study found that CTA head and neck was ordered for 2.5% 8 The VAN (vision, aphasia, neglect) score ( Figure 1 ), first proposed by Teleb et al. of patients with blunt multisystem trauma.
1 The ED is a fast-paced environment where patient stability and life-and-limb-threatening conditions are prioritized. The American Academy of Emergency Medicine has called effective, efficient, and safe pain management a “specialty-defining skill.” Opioid analgesia is appropriate for moderate to severe acute abdominal pain (Table 1).
She describes the pain as left-sided, non-radiating, and 9/10 in severity. The catheterization lab is activated, but catheterization shows no coronary artery occlusion. A 67-year-old female with past medical history of hypertension presents with acute onset of chest pain without associated symptoms. What is the diagnosis?
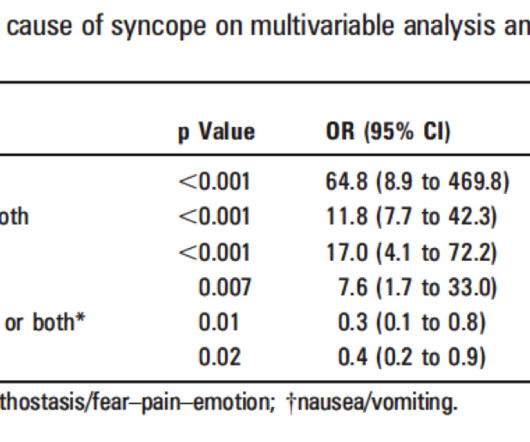
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. It's complicated, but they derived a score based on these variables: 1. h/o heart disease (+1) 3. Troponin greater than 99th percentile (+1) 5.
A 69 year old woman with a history of hypertension presented to the emergencydepartment by EMS for evaluation of chest pain and shortness of breath. The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. This was written by Hans Helseth.
Although these autoantibodies may be present in a variety of individuals, the development of clinical disease is thought to require exposure to an environmental risk factor such as certain viruses, cigarette smoke or other environmental toxins (1). million have been diagnosed with lupus, with 90% of cases occurring in females (1).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content