This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
[link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. cTnI drawn at the same was 0.011 ng/mL (ref.
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. Vital signs include BP 90/48, HR 122, T 98.3
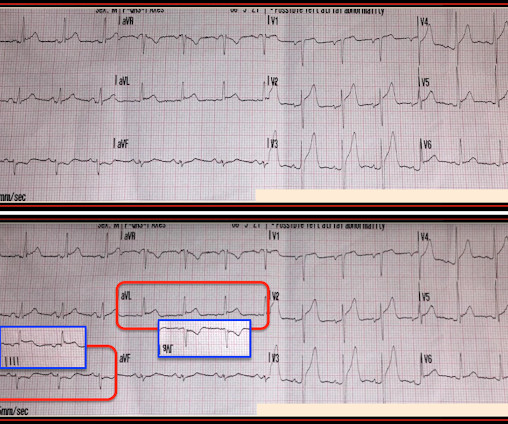
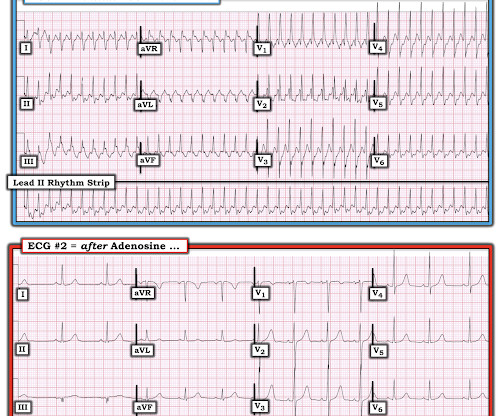
When EMS found her, she was dyspneic and diaphoretic. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Her ECG is shown below: What do you think?
David Didlake, NRP, APRN, ACNP-BC @DidlakeDW Expert analysis provided by Dr. Ken Grauer [link] @ekgpress EMS is called to the main reception area of a retirement center where an elderly female is found down, unconscious and unresponsive. Beats #1-thru-7 manifest the same morphology as we saw in the 12-lead tracing (A) for leads I and II.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ).
Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration.
Pillai, MBBS (@sspillai01, EM Resident Physician, University of Kentucky) and Christopher N. 1 The shortage in supply posed difficulties for hospitals that significantly depend on GE Healthcare as their supplier, which encompassed approximately 50% of hospitals in the United States (US). 11 Table 1. 11 Table 1.
Management must, however, be individualized with respect to the delay to coronary angiography (PCI). Guidelines recommend the use of validated risk models to estimate the risk of acute myocardial infarction , 30-days and 1-year mortality in patients with NSTE-ACS. Circulation. 2000 Oct 24;102(17):2031-7.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
The coronaries were clean (this is not the gold standard, however, as some patients with ischemic ST elevation may have clean coronaries). ACTUAL CORONARY ANATOMY: Dominance: Right LM: A 5 mm vessel which bifurcates into the LAD and LCx coronary artery. QRSV2 = 16 RAV4 = 14 Value = 20.24 (The cutoff of 18.2
He had walked into the ED (did not use EMS). Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Baseline Q-wave surpasses time from symptom onset as a prognostic marker in ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention.
2020;71(1):235-246. Plt 37×10^9/L and 40×10^9/L, SOC and TEG, respectively) All patients enrolled had an upper endoscopy and verified the source of bleeding. Article: Kumar M et al. Thromboelastography-Guided Blood Component Use in Patients With Cirrhosis With Nonvariceal Bleeding: A Randomized Controlled Trial.
He had walked into the ED (did not use EMS). Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. He found 2 ECG patterns of atypical T-wave development in PIRP: 1) persistently positive (upright) T-waves 48 hours after AMI onset. Lessons : 1. J Am Coll Cardiol 53(17):1503-9.
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrial flutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway. See Learning point 1 below.
We’ll keep it short, while you keep that EM brain sharp. She describes the pain as left-sided, non-radiating, and 9/10 in severity. The catheterization lab is activated, but catheterization shows no coronary artery occlusion. Initial vital signs include BP of 157/80, HR of 96, RR 14, SpO2 of 97% on RA, T 37.5.
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University School of Medicine, St. Louis, MO); Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine, St. We’ll keep it short, while you keep that EM brain sharp. A 64-year-old male presents by EMS to the ED with shortness of breath.
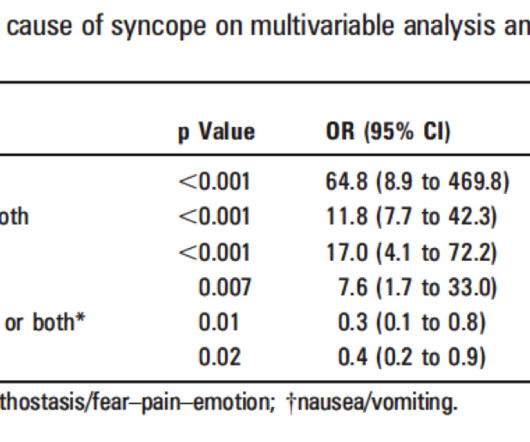
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. Abnormal ECG – looks for cardiac syncope. Syncope without a prodrome, no precipitating factors (EGSYS) 5. Hemoglobin less than 10 (SF rule) 6.
Authors: Mary Hamblen, DO (EM Resident Physician, TX); Justin Hacnik, MD (EM Resident Physician, TX); Katherine Spencer, MD (EM Resident Physician, TX); J.D. 1 One study found that CTA head and neck was ordered for 2.5% 8 The VAN (vision, aphasia, neglect) score ( Figure 1 ), first proposed by Teleb et al.
Bhana, MD (EM Resident Physician, University of Massachusetts/UMass Chan Medical School); Clarence Kong, MD (Pain Fellow, Eastern Virginia Medical School – Virginia Health Sciences at Old Dominion University); Mani Hashemi, MD (EM Attending, HCA Florida Mercy Hospital); S.M. Authors: Nikhil B.
Authors: Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA), Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
Moreover, it does not follow a coronary distribution very well. The coronaries were clean. Today's patient unfortunately developed PEA ( P ulseless E lectrical A ctivity ) arrest shortly after arrival of the medic team. PEA is uncommon as an initial rhythm witnessed by EMS on the scene when the cause is an acute ischemic event.
Pendell Meyers , Aaron E. Puskarich Abstract Objectives Data suggest patients suffering acute coronary occlusion myocardial infarction (OMI) benefit from prompt primary percutaneous intervention (PPCI). PEARL #1: In general, it is rare to see both marked LVH and acute OMI in the same tracing. Figure-1: I've labeled today's ECG.
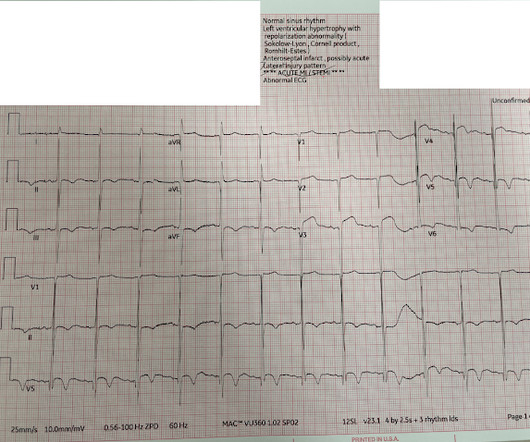
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. This was written by Hans Helseth.
Collins, MD (EM Resident Physician, San Antonio, Texas); Michael J. Although these autoantibodies may be present in a variety of individuals, the development of clinical disease is thought to require exposure to an environmental risk factor such as certain viruses, cigarette smoke or other environmental toxins (1). Authors: William J.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content