This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
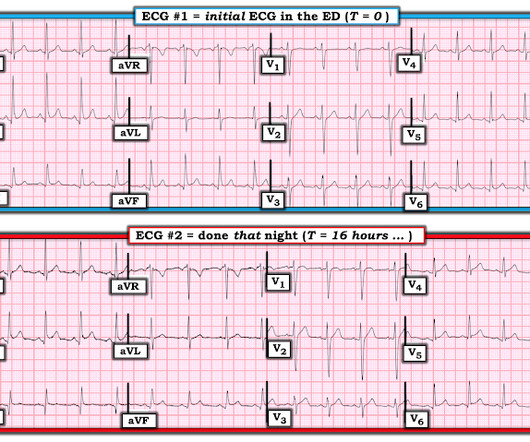
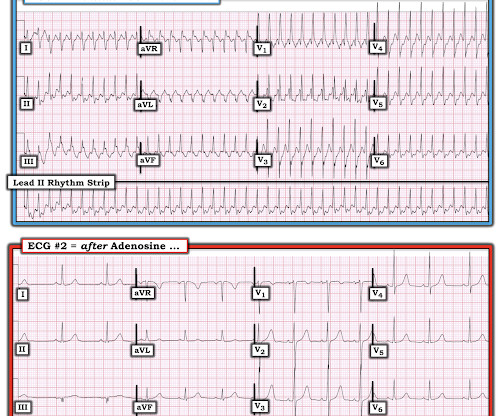
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Coronaries were clean. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. Time is myocardium.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ).
Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration.
1 The shortage in supply posed difficulties for hospitals that significantly depend on GE Healthcare as their supplier, which encompassed approximately 50% of hospitals in the United States (US). 11 Table 1. Preparation 9 Hospitals had to prepare for the impending contrast shortage as soon as potential shortage news occurred.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Takotsubo is a sudden event, not one with crescendo angina. Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chest pain. If there is NO WMA, then it is not coronary occlusion, but if there IS one, then you still don't have a diagnosis.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. As you take another LOOK at ECG #1 — What is the relevance of the findings that I've labeled in Figure-1 ?
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
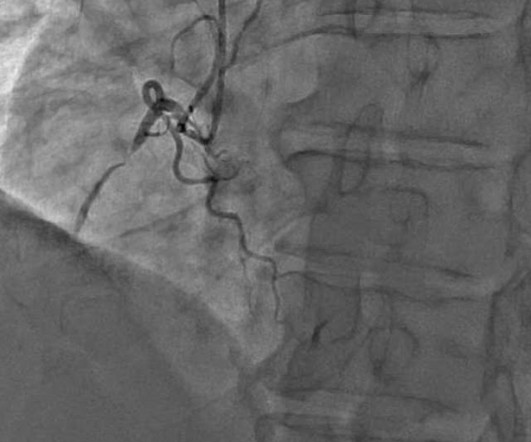
He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent.
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. LEARNING POINT : 1. Along the way to acquiring more experience in recognizing the ECG findings of acute coronary occlusion — is incorporation of a number of KEY ECG Features into one's clinical acumen.
The coronaries were clean (this is not the gold standard, however, as some patients with ischemic ST elevation may have clean coronaries). ACTUAL CORONARY ANATOMY: Dominance: Right LM: A 5 mm vessel which bifurcates into the LAD and LCx coronary artery. QRSV2 = 16 RAV4 = 14 Value = 20.24 (The cutoff of 18.2
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. 25] Stone et al found that 72% have TIMI 0 or 1 flow.
Ct coronary angiogram showed normal coronary arteries. Smith note: I think CT coronary angiogram is reasonable with the elevated troponins and symptoms. Regarding the History: It sounds from the History as if this patient has at least a significant component of EIA ( E xercise- I nduced A sthma ).
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrial flutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway. See Learning point 1 below.
I found a well appearing young lady in the room with her parents who witnessed the event. She denied having any symptoms before or after the event, and she was asymptomatic on my initial exam. She was diagnosed with pericarditis and spent one day in the hospital without events. mm STE depression in aVL. Prac 15(17), 2017.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
This particular facility is situated for independent living, thus no medical providers are on site to provide pertinent details for medical history, medication intake, or remarkable events prior to the incident at hand. Beats #1-thru-7 manifest the same morphology as we saw in the 12-lead tracing (A) for leads I and II.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. So maybe she is better than I am.
And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. In acute MI, the T-wave is large, and the T/ST ratio is high. This is much more typical of myocarditis.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. E CG # 1 = the initial Triage ECG ( TOP ) — As per Dr. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF. As there was ruptured plaque, this is NOT Prinzmetal's angina.
2020;71(1):235-246. Plt 37×10^9/L and 40×10^9/L, SOC and TEG, respectively) All patients enrolled had an upper endoscopy and verified the source of bleeding. Article: Kumar M et al. Thromboelastography-Guided Blood Component Use in Patients With Cirrhosis With Nonvariceal Bleeding: A Randomized Controlled Trial.
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Kirkegaard H, Soreide E, de Haas, I et al. De Fazio C, Skrifvars MB, Soreide E et al. 2019;23(1):1–9.
Learning Points: 1. Smith was asked to interpret without the benefit of any clinical information ( = ECG #1 in Figure-1 ). There are frequent PVCs ( on this tracing — 3 PVCs in the space of 10 seconds = beats #3, 9, 14 ). Thus, the patient may be pain free from infarct alone, even without spontaneous reperfusion.
She describes the pain as left-sided, non-radiating, and 9/10 in severity. The catheterization lab is activated, but catheterization shows no coronary artery occlusion. A 67-year-old female with past medical history of hypertension presents with acute onset of chest pain without associated symptoms. What is the diagnosis?
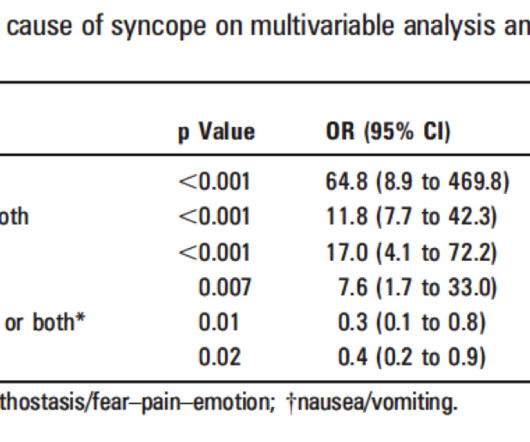
Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. It's complicated, but they derived a score based on these variables: 1. h/o heart disease (+1) 3. Troponin greater than 99th percentile (+1) 5.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. The scan showed a bicuspid aortic valve with severe stenosis and coronary artery disease. The top ECG is diagnostic of thrombotic type 1 OMI until proven otherwise.
Although these autoantibodies may be present in a variety of individuals, the development of clinical disease is thought to require exposure to an environmental risk factor such as certain viruses, cigarette smoke or other environmental toxins (1). million have been diagnosed with lupus, with 90% of cases occurring in females (1).
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. Moreover, it does not follow a coronary distribution very well. The coronaries were clean. Not a shockable rhythm. Resuscitated with chest compressions, epinephrine. This is unusual in acute OMI.
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. The arterial pressure waveform is transduced using the coronary catheter. But in the case of an ostial lesion, there is little or no space between the outside of the catheter and the wall of the coronary artery.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content