This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
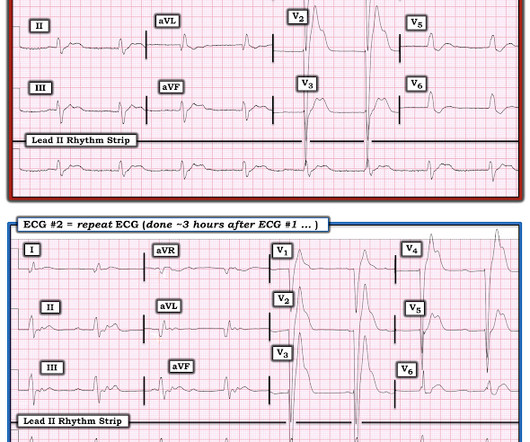
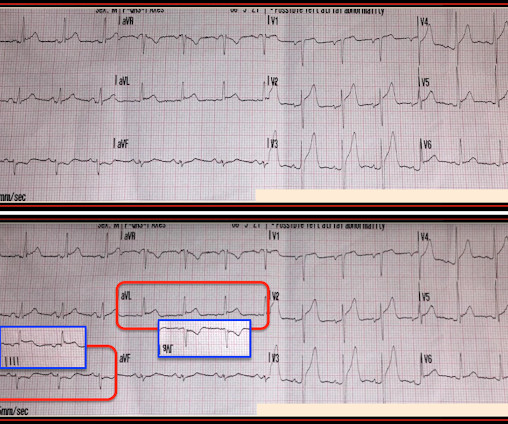
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Coronaries were clean. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. Real or just fake?"
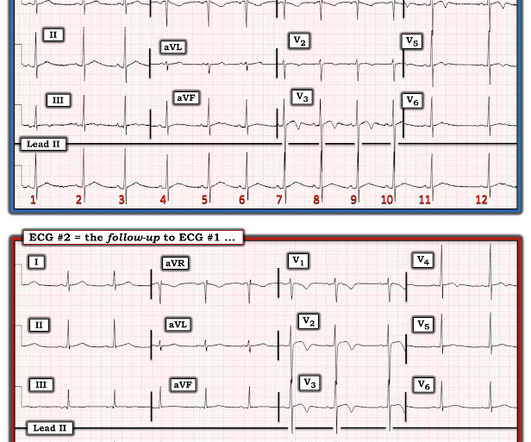
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. While not completely ruling out acute coronary disease — another cause should be considered.
Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. A 12 Lead ECG was recorded secondary to bizarre telemetry findings at bedside. Said differently, it’s a mess.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ).
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. 1 Risk Factors: 1-4 Spontaneous Anticoagulants (Apixaban, Rivaroxaban, etc.)
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. First — Some thoughts on the post -resuscitation ECG.
1 The shortage in supply posed difficulties for hospitals that significantly depend on GE Healthcare as their supplier, which encompassed approximately 50% of hospitals in the United States (US). 11 Table 1. Preparation 9 Hospitals had to prepare for the impending contrast shortage as soon as potential shortage news occurred.
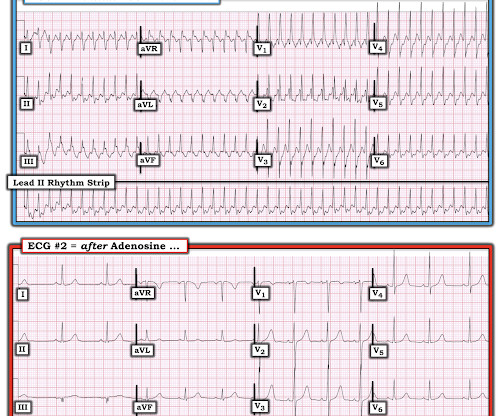
We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. Atropine usually works in junctional rhythm with a narrow complex 9. What is the atrial activity? What to do?
It is unclear to me whether this case could represent 1) simple supply/demand mismatch due to increased demand from epinephrine, 2) Kounis syndrome (usually described as mast cell mediated coronary vasospasm during allergic reaction), 3) brief autolysed left main or LAD ACS with no findings on later echo and CT coronary angio, or 4) something else.
Learning Points: 1. If the situation is not right for acute coronary occlusion, then the ECG findings probably do not represent acute coronary occlusion. Despite the eye-catching ST-T wave changes that came-and-went a number of times — there was no acute coronary occlusion. Figure-1: The first 2 tracings in today's case.
Vittinghoff, E. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. I suggested esmolol if the heart rate did not improve. This would treat both SVT or sinus tachycardia. Later, he was found to have used cocaine. Marcus, G.
The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chest pain. If there is NO WMA, then it is not coronary occlusion, but if there IS one, then you still don't have a diagnosis.
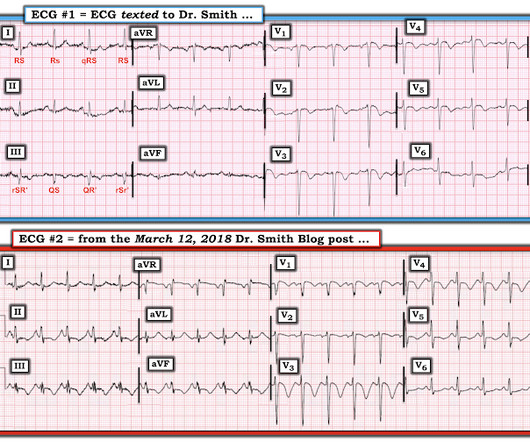
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. As you take another LOOK at ECG #1 — What is the relevance of the findings that I've labeled in Figure-1 ?
Management must, however, be individualized with respect to the delay to coronary angiography (PCI). Guidelines recommend the use of validated risk models to estimate the risk of acute myocardial infarction , 30-days and 1-year mortality in patients with NSTE-ACS. TIMI, GRACE and PURSUIT are such risk models. Circulation.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. V1 has 0.5
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. I’ve excerpted in Figure-1 , relevant paragraphs from a 2017 ESC ( European Society of Cardiology ) article on this subject by Xanthopoulos & Skoularigis ( ESC: Vol. 15-9/6/2017 ). Pericarditis?
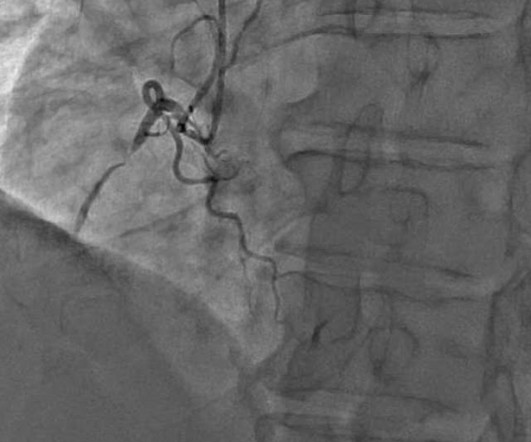
He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent.
The coronaries were clean (this is not the gold standard, however, as some patients with ischemic ST elevation may have clean coronaries). ACTUAL CORONARY ANATOMY: Dominance: Right LM: A 5 mm vessel which bifurcates into the LAD and LCx coronary artery. They gave him water with salt, as he thought he was dehydrated."
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Each small group identified topics, and then the topics were voted on by the entire panel. Instead, target 92-98%.
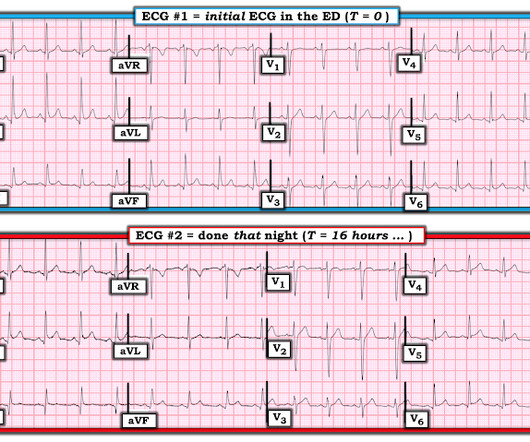
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
mm in just one lead V7-9), but as far as I can tell all of these documents specifically avoid calling this condition STEMI and specifically avoid using any terminology similar to "STEMI equivalent." Here is his triage ECG when he presented at 1657: What do you think? hours after arrival. 1833: Persistent posterior injury.
4 important features that indicate acute right hear strain: 1. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with APE (p less than 0.001). They found that only 11% of PE had 1 mm T-wave inversions in both lead III and lead V1, vs. 4.6%
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. LEARNING POINT : 1. Along the way to acquiring more experience in recognizing the ECG findings of acute coronary occlusion — is incorporation of a number of KEY ECG Features into one's clinical acumen.
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. Tips for recognizing Acute Posterior STEMI: 1. References: 1. This can help in confirmation.
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. 25] Stone et al found that 72% have TIMI 0 or 1 flow.
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 0:00 — Intro by Dr. ) — published by Mayo Clinic CV Podcast Series on 1/16/2024 ( 33 minutes ). speed should be optimal for you!
Ct coronary angiogram showed normal coronary arteries. Smith note: I think CT coronary angiogram is reasonable with the elevated troponins and symptoms. Regarding the History: It sounds from the History as if this patient has at least a significant component of EIA ( E xercise- I nduced A sthma ). What is it?
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrial flutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway. See Learning point 1 below.
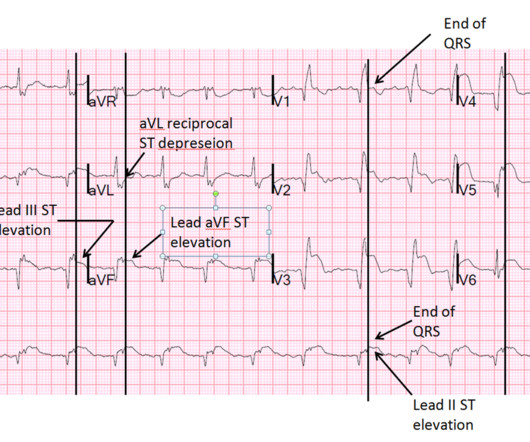
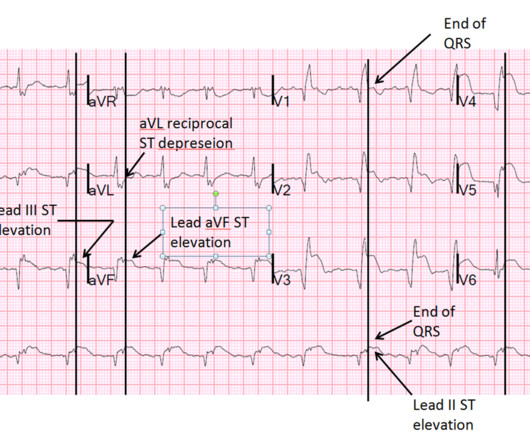
Is this due to coronary occlusion? The medic activated the cath lab but was refused by the interventionalist, who did not believe that this ECG represented acute coronary occlusion. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Why did I say this? Look at aVF.
1 week later (about 1 week prior to the tamponade visit) she had a follow up outpatient visit and this ECG was recorded: Appears to show resolving findings. For an excellent review of the pathophysiological explanation of signs and symptoms associated with Pericardial Tamponade SEE this Review by Jensen et al in the e-Journal Card.
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. Time to know your hs-cTn better.
Moreover , the patient has ongoing symptoms and has an unexplained elevated troponin, so she is having an MI and the only question is whether it is type 1 or type 2 due to hypertension. Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight. At midnight.
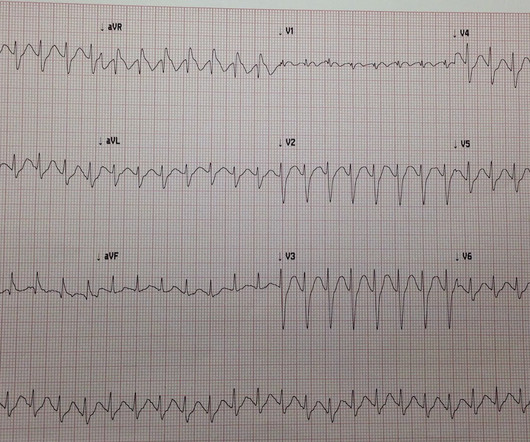
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. PM Cardio digitized version.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. What do you think? In fact, Kosuge et al. Stein et al.
And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. In acute MI, the T-wave is large, and the T/ST ratio is high. This is much more typical of myocarditis.
Most agents exhibit both vasopressor and inotropic effects (Figure 1). Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). μg/kg/min + + + ++ Low dose dopamine stimulates D1 receptors and induces vasodilation in coronary, renal, cerebral and mesenteric vessels.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Suppose you had used the formula?
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Baseline Q-wave surpasses time from symptom onset as a prognostic marker in ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention. J Am Coll Cardiol 53(17):1503-9. Could it be acute (vs.
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. He found 2 ECG patterns of atypical T-wave development in PIRP: 1) persistently positive (upright) T-waves 48 hours after AMI onset. Lessons : 1. Although rupture has a high mortality, it is not uniformly fatal References 1.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content