This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
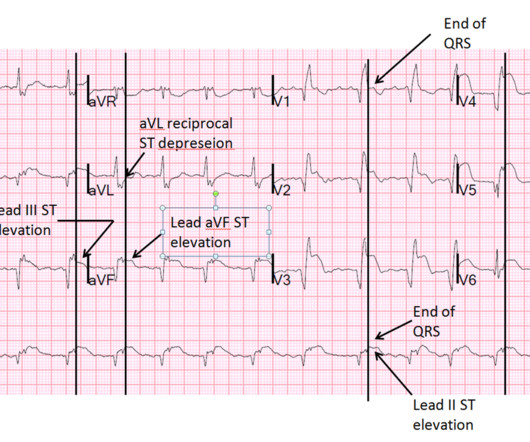
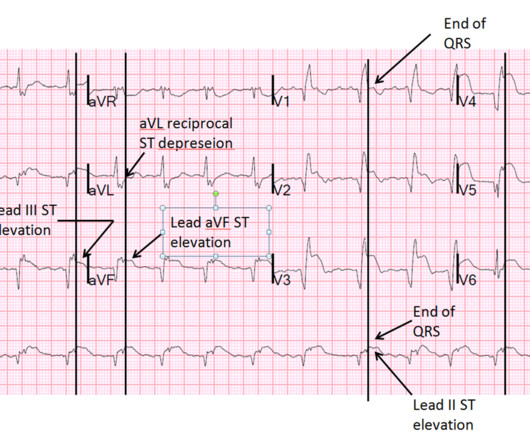
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Figure-1: I've labeled the initial ECG in today's case.
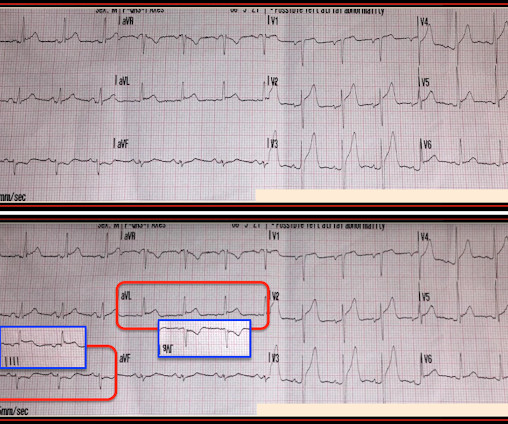
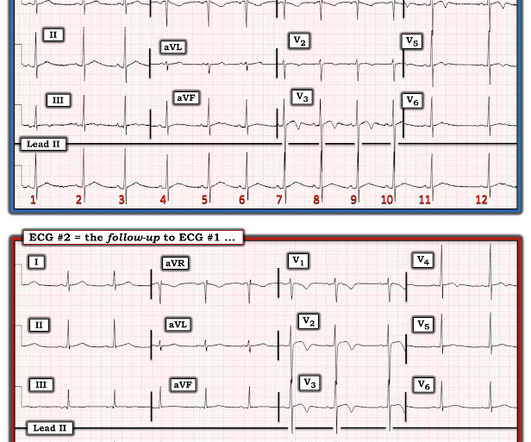
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." found normal ECGs in only 3 of 50 patients with massive PE, and 9 of 40 with submassive PE.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. PM Cardio digitized version.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Figure-1: The initial ECG in today's case — obtained after ROSC.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Management must, however, be individualized with respect to the delay to coronary angiography (PCI). Guidelines recommend the use of validated risk models to estimate the risk of acute myocardial infarction , 30-days and 1-year mortality in patients with NSTE-ACS. Circulation. 2000 Oct 24;102(17):2031-7.
There is an obvious inferior posterior STEMI(+) OMI. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. What is the atrial activity? How would one tell? What to do?
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Lessons : 1.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. No TIMI flow was listed in the report.
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
A "STEMI alert" was called and soon cancelled. Comment by K EN G RAUER, MD ( 3/1 /2023 ): = Today's case by Dr. Meyers serves as a reminder of the important clinical entity known as diffuse subendocardial ischemia. ST depression will not always be present in 9/12 leads — as is seen in Figure-1.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. What do you think?
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF. Why is this important?
And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 Angiogram was negative.
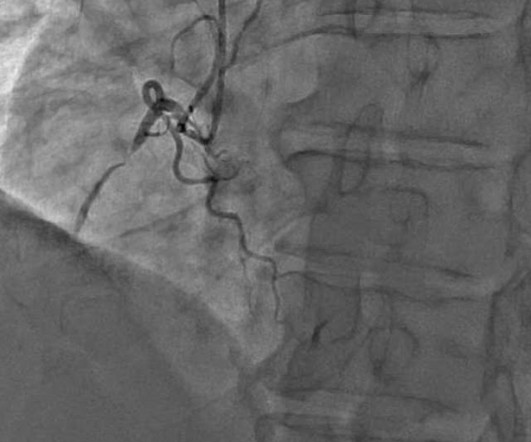
He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent.
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. Rather than using terms like “STEMI” and “Wellens”, it’s more helpful to describe the underlying pathology and ECG pattern pattern: Occlusion MI, and reperfusion T wave inversion 4. JAMA Intern Med 2019 9.
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? 15-9/6/2017 ). Pericarditis?
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 0:00 — Intro by Dr. ) — published by Mayo Clinic CV Podcast Series on 1/16/2024 ( 33 minutes ). 9:25 — Are there hyperacute T waves?
Is this due to coronary occlusion? The medic activated the cath lab but was refused by the interventionalist, who did not believe that this ECG represented acute coronary occlusion. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Why did I say this?
Ct coronary angiogram showed normal coronary arteries. Smith note: I think CT coronary angiogram is reasonable with the elevated troponins and symptoms. Anterior STEMI? Regarding the History: It sounds from the History as if this patient has at least a significant component of EIA ( E xercise- I nduced A sthma ).
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial.
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Learning Points: 1.
Angiogram showed a 99% left main thrombotic occlusion with TIMI-1 flow (this is considered "occlusion" even though there is some flow. not left main occlusion == MY Comment by K EN G RAUER, MD ( 1/16/2020 ): == I did not correctly identify the “culprit artery” in this case. mEq/L Her BP with pressors came up to 80, then 100.
1 week later (about 1 week prior to the tamponade visit) she had a follow up outpatient visit and this ECG was recorded: Appears to show resolving findings. For an excellent review of the pathophysiological explanation of signs and symptoms associated with Pericardial Tamponade SEE this Review by Jensen et al in the e-Journal Card.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. Moreover, it does not follow a coronary distribution very well. From this site.
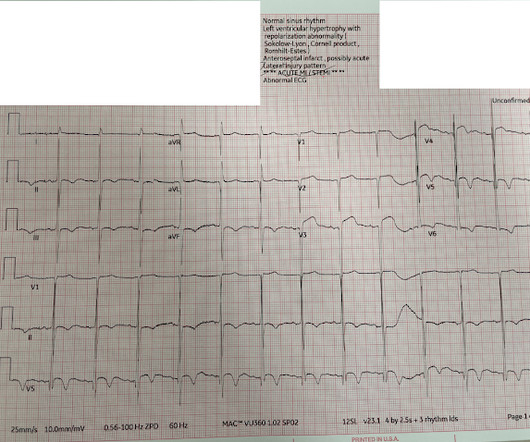
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Pendell Meyers , Aaron E. I suspect most blog readers did not struggle with this one. Baker , Shifa R.
Whether your program is primarily 9-1-1, interfacility transport (IFT), or a combination of both, the likelihood of being responsible for the safe and expeditious transport of a STEMI patient is high for anyone in the out-of-hospital care setting. There, we would find two coronary ostias, left and right.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Also see these posts of Type II STEMI. An EKG was immediately recorded.
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. The arterial pressure waveform is transduced using the coronary catheter. But in the case of an ostial lesion, there is little or no space between the outside of the catheter and the wall of the coronary artery.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content