This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. You (or someone in your department) needs to know which assay your ED has, and use the appropriate values for that assay.
Case: You are working a busy shift in a rural emergencydepartment (ED) and your excellent Family Medicine trainee presents a case of a 63-year-old woman with chest pain and some intermittent radiation into the inter-scapular region. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia.
The Case A 41-year-old male presents to the ED with constant palpitations for one day. Risk factors that increase the likelihood of VT include history of previous myocardial infarction, known coronary artery disease, and structural heart disease. When in doubt, treat as ventricular tachycardia.
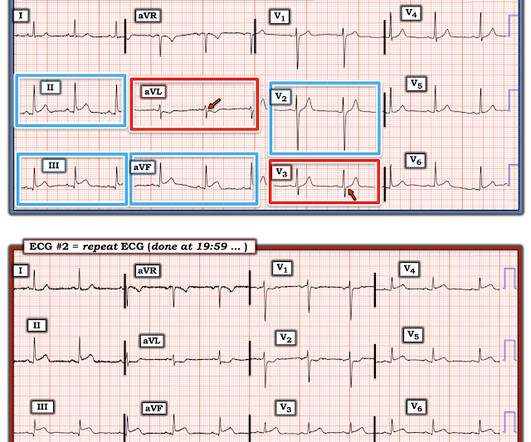
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Andrew Huang: Andy is […] The post SGEM#280: This Old Heart of Mine and Troponin Testing first appeared on The Skeptics Guide to Emergency Medicine. Reference: Wang et al.
Kaushal Khambhati is also a fourth-year resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. She has a history of hypertension and non-insulin dependent diabetes mellitus.
He is a GP by training but works in EmergencyDepartment, Anaesthesia, Internal Medicine and Paediatrics. He has a wonderful #FOAMed blog and podcast called Broomedocs and also work […] The post SGEM#326: The SALSA Study: Hypertonic Saline to Treat Hyponatremia first appeared on The Skeptics Guide to Emergency Medicine.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." But troponin is a rear-view mirror which shows damage that has already occurred, and is often within the normal range within only 2 hours of onset of acute coronary occlusion.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The patient was rushed to the nearest emergencydepartment (non-PCI facility) for stabilization.
Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment. Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. What do you think?
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Annals of Emergency Medicine 2011; Suppl 58(4): S211.
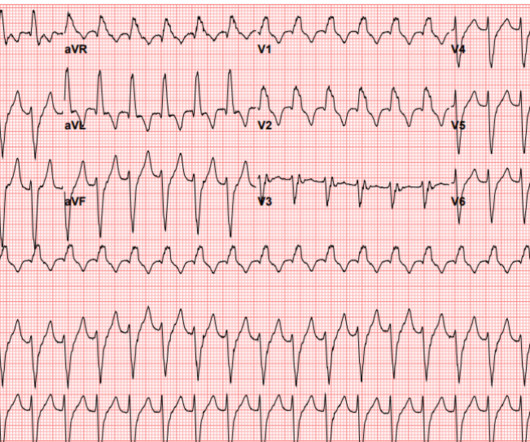
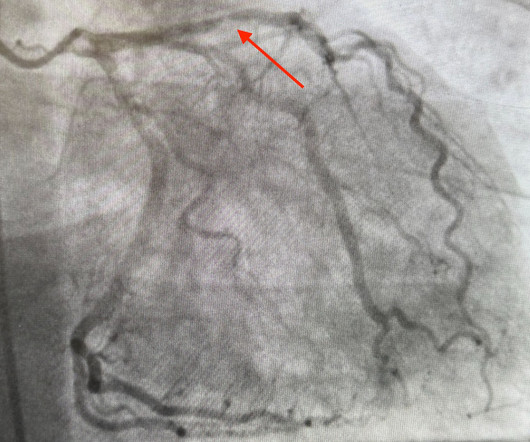
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram. link] [1] Mirand, D.
The specific ST/T pattern was not fully appreciated by the attending EMS personnel, yet alarming enough to convince the patient to be seen in the EmergencyDepartment despite his intentions of seeking evaluation on his own accord through his respective family physician. But the lesion is still active! MICU transport was unremarkable.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Patient not informed of enlarged heart, dies 3 weeks post ED visit Miscommunicated radiology findings are a hot topic. Someone should have – either the first ED doc, the second ED doc, or my PCP.
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment. Am J Emerg Med.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. STEMI vs. NSTEMI dichotomy is not sensitive for true occlusion MI or acute coronary occlusion. J Am Coll Cardiol.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. Adult cardiac arrest in the emergencydepartment – A Swedish cohort study.
It is commonly used in EmergencyDepartments, especially in febrile and possibly infectious patients. Take Home In the ED, CRP should not be used to make a diagnosis but to assist evaluation and support your clinical suspicion. In clinically unwell patients, a normal CRP level should never delay antibiotic coverage in ED.
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). link] ] Outcome The patient emerged neurologically intact. Clinical Cardiology 2019.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergencydepartment patients. Western Journal of Emergency Medicine, 18 (4), 752-760. [2]
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. The undergraduate is now willing to identify himself: Hans Helseth. No ECG was ordered on Day #1.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Guagliumi, G., Iwaoka, R.
Upon arrival at the receiving emergencydepartment, however, she precipitously degenerated into VF and could not be resuscitated. In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Chou’s Electrocardiography in Clinical Practice (6th ed).
She presented to the emergencydepartment after a couple of days of chest discomfort. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). This patient presented to the ED “after a couple of days of chest discomfort”.
Belcher, MD (EM Attending Physician, University of Kentucky, Department of Emergency Medicine) // Reviewed by: Jessica Pelletier, DO (EM Education Fellow, Washington University School of Medicine); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) “What do you call an IV contrast shortage? Alternative contrast agents.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. EKG on arrival to the ED is shown below: What do you think? Blood glucose was not low at 162 mg/dL.
AslangerE A 65-year-old gentleman presented to the emergencydepartment after experiencing two recent ICD shocks in the preceding hours. A recent angiogram report indicated a totally occluded left anterior descending artery (LAD) and right coronary artery (RCA), with 30-40% narrowings in the left circumflex artery (LCx).
But the paramedic and the ED physician in this case did not subscribe to this idea. Am J Emerg Med. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. 2022 Jan;51:384-387.
A 50 year old presented to the emergencydepartment of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chest pain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. Figure-1: The first 2 tracings in today's case. The Need for Immediate Transport?
Many systems now refrain from showing computer "normal" ECGs to the busy emergency physicians at triage because of very poorly conceived articles that say that if the computer algorithm says "normal," the emergency physician should not be bothered. It is clearly missed by the conventional algorithm.
2, 3 Biliary POCUS can help decrease patient length of stay in the EmergencyDepartment. 2, 3 Biliary POCUS can help decrease patient length of stay in the EmergencyDepartment. Utility of common bile duct measurement in ED point of care ultrasound: A prospective study. Am J Emerg Med. 2022;7:188-189.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. In the ED, his troponin, ECG, and chest X-ray (CXR) are normal. He survives.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 FIGURE 1: First ED EKG. FIGURE 2: Baseline ED from 2 months prior. FIGURE 3: Second ED EKG. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn. Click to enlarge.)
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergencydepartment (ED). The patient initially presented to an outside ED and was subsequently transferred to our facility for continuity of care.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Here is the first ED ECG, with no pain: Sinus rhythm. Akkerhuis KM, et al.
She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. BP gradually rose. Results: Over 8.5
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content