This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Upon EMS arrival, they find the patient is sweaty with normal vital signs. AEM November 2023. AEM November 2023.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
David Didlake @DidlakeDW EMS personnel responded to the residence of an 81 y/o Male with syncope. At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. The ED activated trauma services, and a 12 Lead ECG was captured. This was deemed “non-specific” by the ED physicians.
Sepsis) De Winters T waves are the earliest sign of an anterior wall MI but will only be present in ~ 2% of LAD infarcts Patients with Wellens Syndrome on ECG should have a cardiac cath within 24 hours, not necessarily within the first 60 minutes of ED arrival.
We’ll keep it short, while you keep that EM brain sharp. A 3-year-old male with no past medical history presents to the ED with one week of daily fevers >102°F associated with four days of rash on the trunk. Tomisaku Kawasaki, who noticed 50+ similar pediatric presentations between the years 1961 and 1967.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. Vital signs include BP 90/48, HR 122, T 98.3
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification. Cardiol Rev.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think?
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. It’s judicious, then, to arrange for coronary angiogram.
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. Below is the initial ED ECG.
EMS arrived and found him in Ventricular Fibrillation (VF). The patient was brought to the ED and had this ECG recorded: What do you think? The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia.
EMS personnel found him seated on a bench, uncomfortable, but without gross distress. A second 12 Lead ECG was recorded: This is a testament to the dynamic nature of coronary thrombosis and thrombolysis. He waited for it to subside, but after 30 minutes of persistence he called 911. But the lesion is still active!
We’ll keep it short, while you keep that EM brain sharp. A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. Post TW, ed. hour IV thrombolytic window.
The Case A 96-year-old female with a history of coronary artery disease, hypertension, and complete heart block status post dual-chamber pacemaker (remote) presents to the ED by EMS with generalized weakness and lethargy. This rhythm will not result in cessation with magnet application.
The Case A 96-year-old female with a history of coronary artery disease, hypertension, and complete heart block status post dual-chamber pacemaker (remote) presents to the ED by EMS with generalized weakness and lethargy. This rhythm will not result in cessation with magnet application.
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. Ultimately the patient went to Cath and was found to have multi-vessel obstructive coronary disease with an acute LCX culprit vessel, which was stented.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Here is the LAD after stent placement.
EMS finds him supine, alert and oriented, and without any gross distress. He advises, however, recurrent syncopal episodes for the past six months, some of which have resulted in ED admission, yet no identifying mechanism could be determined. It’s reported that he regained consciousness after 30 seconds, approximately.
EMS found her acutely ill, mottled, dry mucous membranes, modestly hypotensive, and lethargic. This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2]
Fire/EMS crews found him clammy and uncomfortable. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Learning points 1] Acute Coronary Syndrome has many shades of clinical manifestation.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. Patient received 11 shocks by ICD and was in V-fib when EMS arrived.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
The machine indicated STEMI (but it barely meets STEMI criteria, if at all) and the patient was brought to the ED: On arrival 20 minutes later the pain had reduced to 1/10 after aspirin, and the patient had repeat ECG at triage: Now the ST segments and T waves have normalized, and the only abnormality is sinus bradycardia and loss of R waves.
He called EMS who brought him to the ED. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. ED Diagnoses: 1. This patient in today's case was a man in his 60s with a known history of coronary disease, including prior stents.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Clinical Cardiology 2019.
He reported to EMS a medical history of GERD only. 1] Here is the admitting ED ECG after cancellation of Code STEMI. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. The patient continued to verbalize cessation of symptoms while in the ED.
Episode 86: Tricky Cases Part 2 Case 3: 56-year-old female with history of seizures, actively seizing, EMS called. Patient seized for approximately 20 minutes prior to EMS arrival. On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Every airway requires a plan and backups.
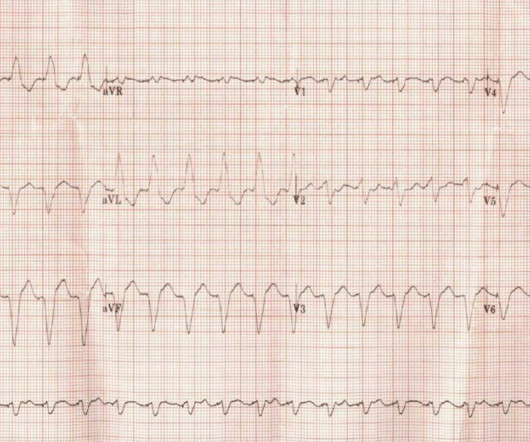
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram. 5] Surawicz, B.
David Didlake, NRP, APRN, ACNP-BC @DidlakeDW Expert analysis provided by Dr. Ken Grauer [link] @ekgpress EMS is called to the main reception area of a retirement center where an elderly female is found down, unconscious and unresponsive. She has a palpable pulse at the radial arteries, bilaterally, with shallow respirations.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. This is not the case.
When EMS found her, she was dyspneic and diaphoretic. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Objective: Based on current evidence, this review article aims to guide the Emergency Department (ED) in providing care for patients with blast injuries. Cardiovascular: Injury: cardiac contusion, wall rupture, tamponade, papillary muscle rupture, valve injury, aortic arch injury, and coronary artery dissection.
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). Chou's Electrocardiography in Clinical Practice, 6th ed. link] [1] Zachary et al.
AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain. He doesn’t have any specific symptoms today, including no fever, vomiting, diarrhea, or urinary symptoms.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Patient not informed of enlarged heart, dies 3 weeks post ED visit Miscommunicated radiology findings are a hot topic. Someone should have – either the first ED doc, the second ED doc, or my PCP.
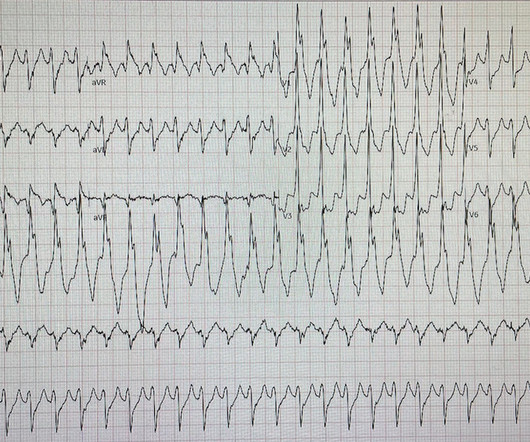
Past medical history includes coronary stenting 17 years prior. Initial ED ECG: What do you think? Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. How Can We Prove that ECG #1 is VT?
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease.
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. Coronary artery disease in patients with out-of-hospital refractory ventricular fibrillation cardiac arrest. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S. Circulation. 2019;139(12):e530-e552.
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL.
Objective: Based on current evidence, this review article aims to guide the Emergency Department (ED) in providing care for patients with blast injuries. Cardiovascular: Injury: cardiac contusion, wall rupture, tamponade, papillary muscle rupture, valve injury, aortic arch injury, and coronary artery dissection.
He awoke from sleep with crushing central chest pain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery. de Zwaan C.,
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. What do you think? In fact, Kosuge et al. Accessed May 28, 2024.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content